
Reducing post op sensitivity and visits with this software function

Rich Rosenblatt did a great post about the articulator function and using it when doing implant crowns. Here is the link: https://www.cerecdoctors.com/discussion-boards/view/id/53970
It got me thinking about something I have been doing regularly.
About 8-9 months go I started a little experiment in my office. I started using the articulator function that is built into the software. My reason for doing this was two fold. First I wanted to see how accurate the articulator is and also to see if it would reduce my post op adjustment.
As a lot of us have come to realize e.max does not mark very well with articulating paper. That coupled with a numb patient make it hard to see excursive interferences. The topic of post op sensitivity with e.max comes up pretty regularly on the cerecdoctors.com boards and inevitably, after the recommendation of checking the occlusion for interferences, the sensitivity goes away after adjusting. This got me thinking about using the articulator to find these problem areas so that we wouldn't have to have the patient calling back with post op sensitivity and needing an adjustment.
This is also an advantage when dealing with zirconia. Adjusting zirconia is not only difficult but also it is imperative that the zirconia gets brought back to a good polish to prevent wear on the opposing dentition. So the less we have to adjust the better, especially since we can't try it in until it after it is sintered.
Here is a case that shows the use of the articulator. This patient has an anterior open bite and group function. If we did not take into account the excursive movements then the chance of an interference is high. Which of course will lead to a need for post op adjustments and more chair time.

This first step is to make sure the articulator is active. This is done by going to Configuration->Pptions->Articulator and checking the active button under use articulator. I do not use the articulator to get my proposal, I just have it active to be able to use the articulator. Once this is done any case you open up will be able to have the articulator turned on. This is done in the Administration phase.
To use the articulator function and have it be accurate you need to image to the canine. Which is what I did until recently. Now that it is advantageous to image to the mid-line, I go ahead and image to the contra-lateral canine. This helps set the model axis by making it easier to set the curve of Spee and Wilson. This will give us a better initial proposal and sets the articulator up properly for the best result.

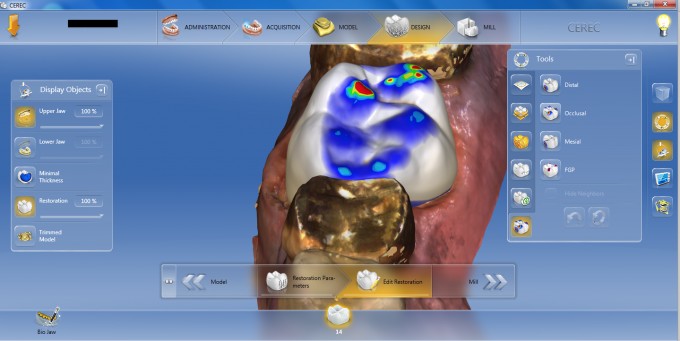
Once the initial proposal is given the distal marginal ridge is slightly lower than ideal.

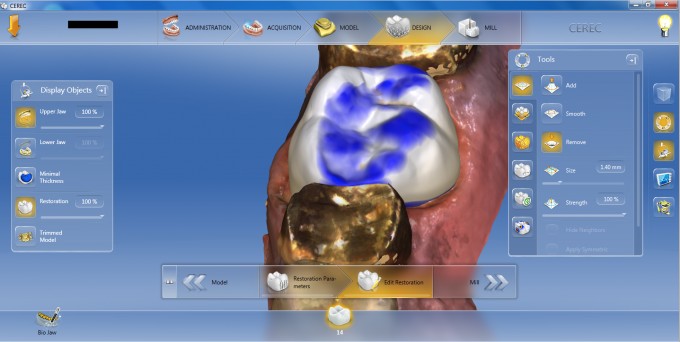
This is quickly adjusted by using the 4 Direction Anatomical Shape tool. This ends up raising the occlusion to much and needs to be adjusted.

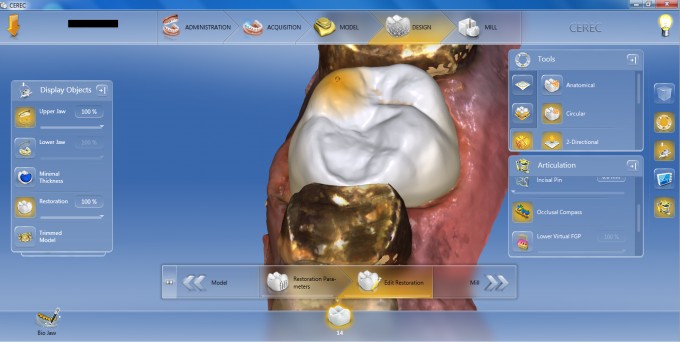
Once adjusted the proposal looks pretty good and should be ready for the milling chamber.
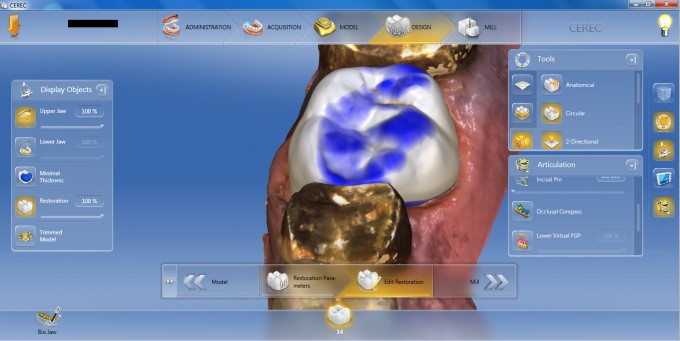
However if we turn on the occlusal compass we can see where we will have interferences that will lead to post opertative sensitivity. The Occlusal Compass is found under the Articulator menu.
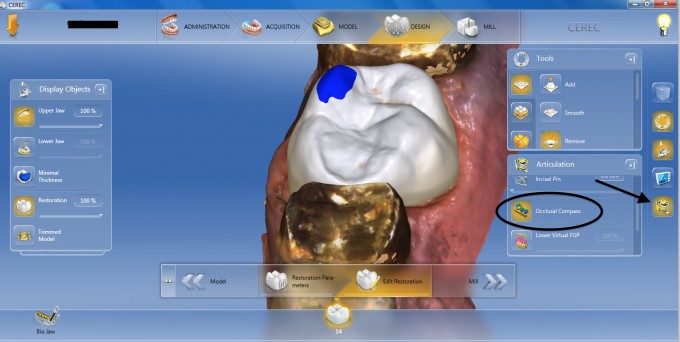
Once the compass is turned on you will see the areas that are hitting in the various movements. You can turn of each of the various interferences to see which ones are present and which are not. Then use whichever tool best fits to make the appropriate adjustment. In this case the 2 directional circular shape tool is used to reduce the height of the cusp.
This gets rid of all the excursive interferences. The compass is turned off and the regular occlusal map is visible again.
As I stated earlier I started doing this about 8-9 months ago and have seen a drastic decrease in post op adjustments and sensitivity. By using the articulator to reduce the amount of interferences you can decrease the number of post op visits and occurrence of sensitivity for your patients.
The long and the short of it is use the articulator function for better results on every type of case.


Excellent. Will start to use this feature. Makes perfect sense. Great that you have noticed less sensitivity. I think you have discovered a "hidden" pearl in our quest for decreased Cerec sensitivity.


Thanks! I have just been now been seeing some my first round of cerec patients for recalls and we have a small batch complaining of sensitivity. I will def be incorporating this.
Thanks!


Nice OB. I agree. It has been working very well here too. I seem to be imaging more often to the contralateral canine unless I'm doing biocopy. Nice explanation of the tool.



On 2/7/2017 at 7:28 am, Mike Skramstad (Faculty) said...Use it on every single case.
I have too skram. Do you find yourself imaging just to mid line or to the contralateral canine? I have been doing it with good success imaging to the midline since you said it does not matter much. wondering if your mind has changed on this


Nice Darin! I assume you are using the default numbers for the various adjustments on the articulator for cases like these?

Great post that makes a lot of sense. You are right, its hard to see the paper marks well in the mouth. Less adjustment in the mouth better it is for the patient's as well as dentist's health. ![]()
On 2/7/2017 at 8:17 am, Richard Rosenblatt said...On 2/7/2017 at 7:28 am, Mike Skramstad (Faculty) said...Use it on every single case.
I have too skram. Do you find yourself imaging just to mid line or to the contralateral canine? I have been doing it with good success imaging to the midline since you said it does not matter much. wondering if your mind has changed on this
It will be more accurate if you image to the contralateral canine... but it still work fine just imaging to midline.
By imaging to the contralateral canine you will have more accuracy in non working interferences but working side interferences will be good if just images to the midline
On 2/7/2017 at 10:01 am, Brian Saltzman said... just used it for a zirc crown on #18 and the bite was spot on!!!
That is awesome. Glad it helped out so quickly.

I hate to sound like a dinosaur, but does this work with Bluecam and 4.3? It does have articulation function, but I dont think it works as you described.

Great information. 2 questions.
1. Do you image to the contra-lateral canine on the opposing arch as well?
2. Why don't you recommend using it to get your initial proposal?
Thanks in advance.
On 2/7/2017 at 11:22 am, Michael Saso said...I hate to sound like a dinosaur, but does this work with Bluecam and 4.3? It does have articulation function, but I dont think it works as you described.
Michael it works but imaging to the midline or contralateral does not help with proposals, since that was introduced with biojaw in 4.4. But the articulator should work just fine.
On 2/7/2017 at 11:53 am, Andres Gamboa said...Great information. 2 questions.
1. Do you image to the contra-lateral canine on the opposing arch as well?Yes I do. Otherwise you won't get the canine guidance if it exists for that side.
2. Why don't you recommend using it to get your initial proposal?I am playing with it to see if it makes a huge difference or not. Stay tuned.
Thanks in advance.
Answers in RED above.
Darin,
Where are you taking the BB in these cases? I have noticed sometimes if I take it in the posterior if imaging to the contralateral canine sometimes give a faulty bite. If I image the anterior 4 teeth for the bite it seems to work better. Just wanted to know your experiences. Im sure Mike will chime in as well.
Tom
I tend to take it in the premolar region. How you construct your model is actually more important than where you take the bite. Construct it in a linear fashion, similar to the ortho software. I then take the buccal bite in the premolar region and roll the camera to capture the gingiva, embrasures and even a bit of the occlusion as well
