
Cerec crown treatment planning

At our staff huddle today, the discussion was on patients that had been treatment planned for Cerec crowns and ideally needed crown lengthening to make room and get good food shedding characteristics. Some patients in the past, for one reason or another, elected not to do the Cerec crown on the basis of having to have another procedure done prior to the crown prep. The one patient in question was a female patient in her 40's who can definitely be classified as a 'bruxer.' #31 on the distal marginal ridge was worn down level to the marginal gingiva (or maybe 1/2 to 1mm above.) I told staff, "I need to get at least 1.5 mm reduction on the occlusal in order to make room for strength for the Cerec crown. Maybe the best thing to do is not treatment plan this tooth for a Cerec crown if patient can't accept crown lengthening as part of the therapy and just do an all metal crown which my lab man says we can work down to 0.3 mm."
What is this Forum's thoughts on this problem? Thanks

As they say just because you have an "omellete maker doesn't mean you have to eat omelletes every day". If you don't think you can make a CEREC crown work than use full cast crown in this case. Absolutely nothing wrong with that option. Believe me there will be plenty of Cerecs to do down the road. By the way eMax is just fine at 1mm thickness. Oh and check this particular patient for sleep apnea as well. The bruxing could be part of the equation along with acid reflex.
Sure you can cast a metal crown with 0.3 mm thickness, but if you put a 0.3 mm thick metal crown on a bruxer, I believe they will eat right through it and then you'll have to deal with a hole in the crown. I'm sure I can mill one that thin too, but it will fracture.
Personally I wouldn't feel comfortable placing a crown of any material on a bruxer without adequate thickness for longevity of the selected material.

It may be easier on you and your staff if you adapt a true digital workflow for all of your crowns. I hate to see an office get into the habit of calling crowns "CEREC crowns". It puts a negative slant on the process. The team needs to be excited and not dread the procedure. They are all crowns, it just depends on how they are manufactured.
Book every crown patient with the intent of delivering same day. Prep as you see fit. Image, design and then make the decision as to whether or not is it appropriate to mill the crown in office. If you don't have adequate thickness just hit the CONNECT button at the top of the screen and send it to the lab for PFM, gold, zirconia or whatever material you'd like. Now mill the temporary crown. The patient will be impressed by your technology as well as your attention to detail. It takes the staff out of the decision-making process.

I think there is a folly of logic at play here. As a Cerec clinical trainer, I hear these statements about tooth reduction all the time with regard to gold and zirconia needing less reduction than e.max. Unfortunately, what is happening is that we are trying to apply old logic to new materials instead of realizing that true adhesive materials like e.max create a new paradigm and some of the old principles can be let go.
With that in mind, let's walk through the considerations. Can gold and zirconia be thinner than e.max occlusally? It's debatable, but for argument's sake, let's say "yes". But since gold and zirconia cannot be reliably bonded, they need axial reduction for conventional resistance/retention form. So you end up taking more tooth structure for those materials, it's just on a different tooth surface. The major drawback is that you are taking away tooth structure on the axial wall plus some vertically at the gingival margin to achieve the proper ferrule for resistance/retention of a non-bonded restoration. In essence, you are taking an already short tooth and fighting to get vertical prep height (aka ferrule) after you make it shorter by prepping it 360 degrees. This vertical prep requirement is what leads you to need crown lengthening. You need to make the tooth longer so you can get more retention/resistance. It's a counter-intuitive and unintended consequence of your material choice.
On the other hand, let's think about an e.max prep. Since I can adhesively bond e.max, all I need is adequate occlusal reduction and clearance. I don't need ferrule or axial reduction at all, as long as I have some enamel to bond to at the restorative margin (which I will have since I don't have to axially reduce the tooth). So with this non-retentive prep design, as long as I'm not going to hit pulp by reducing occlusally 1.5-2mm, I have everything I need for long-term bonded success. I've done a ton of e.max on molars using these prep priciples, and I have never hit a pulp and I can't recall a single case of needing crown lengthening.
So, in short, do I possibly take away a little more occlusally so that I don't have to prep axially or have a vertical ferrule requirement? Yes. Do I have frequent dislodged restorations, cracked/perforated crowns, or post-restorative endo complications? No, only very rarely...actually a small fraction of the average reported in the literature.

Ross gave a great explanation. Let me add that a 2nd molar with tissue almost up to the marginal ridge can generally easily accomodate not only the occlusal reduction, but if needed some axial reduction on the distal as well, without needing crown lengthening. True crown lengthening is a boney procedure, typically to avoid biologic width issues. Anything else is gingivoplasty. The prep for that tooth probably has no need to get anywhere near to the CEJ. Tissue does not attach to enamel, so unless it is partially impacted is rare that a lower molar has anything more than soft tissue on the distal that needs to be managed. That could mean a distal wedge to lower the tissue, or sometimes just a bit wider troughing with the laser to get the margin exposed for imaging and bonding. If the margin ends up subgingival after it recovers, who cares?

+100000 for Ross's post. Excellent!
I will add to this discussion as its been a bit of a issue that I am passionate about so I hope you all will give me the leverage to rant a bit. Dentistry is hard. Its a diffcult profession. We have to work within very small tolernaces, we have patients who would absolutely would rather be anywhere but our chairs. Yet despite these challenges that are already present, we make things even more difficult for ourselves unnecessarily.
Take the example of a broken down tooth with subgingival decay. We work hard to clean out the decay. We work hard to isolate the tooth We work hard to image a deep margin. We work hard to design the case and then bond it in less than ideal circumstances. Then we go home overly tired complaining about the dental profession and how difficult it is. We get even more stressed when despite all the hard work the case fails and now we have an upset patient becuase what should have happened from the get go is crown lengthening on the tooth.
Step back for a second and look at the scenario and ask who created the diffcult situation above. Why was the procedure more difficult than it needed to be? Because we did not do what should have been done- in this case, crown lengthing prior to the crown prep.
Why would we not offer ideal treatment for the patient from the start? If the decay is deep and margins are going to be difficult to isolate- why not do crown lengthening? I mean, if you really want to do it as well as possible, crown lengthening will be needed and the entire case becomes much easier. I will argue why would you even consider doing the case if the patient wont do it properly? Infact, how does the patinet even aware that the crown lengthening is even optional? Think about that for a second.
You say the patient did not want to do crown lengthening prior to a crown. My question to you is how does the patient even know that is an option? Does the patient have any dental background? No obviously not but somehow they have the impression that to treat the tooth we the opportunity to do the crown with the crown lengthening or without. If you are the patient- think about which scenario you would select?
The reason they feel that a crown is possible without crown lengthing is because that was given to them as an option by someone in the dental office. If you dont believe in doing the most ideal treatment, then your team members wont beleive and if the team does not believe in the treatment how are you going to convince the patient to get the treatment done.
Your patients did not go to dental school. You did. Your patients dont know right from wrong. Its your job as a professional to guide them to do the best treatment to take care of their teeth.
Go to your cardiologist and say- listen, I dont really feel like getting the angioplasty for the 95% blockage in my artery. Just give me some medication instead. What do you think they will tell you? Good luck with that discussion.
Lets look at another example- deep decay in a tooth. You make the appointment more stressful by trying to "avoid a root canal" becasue the patient said they didnt want a root canal. Again- sabotage to yourself. You are stressed trying to accomplish the patients wishes. The patient is anxious because you told them that you will try not to do a root canal- as if you have any control over that. Dentistry is no longer fun when we have to deal with situations such as these. The proper thing to do is to tell the patient exactly what is going on and if the tooth needs a root canal, it needs a root canal. The improper thing is to try to do treatment based on the patients desires- not the clinical outcome of the case.
Granted there are bigger issues that play into all of this- patient finances, expectations, availability of specialist if needed. Yada yada yada I get it. But the biggest piece that education and experience has taught me is to not compromise. Yes some patients will leave but many more will find you because of your thorough nature and lack of complications.
Why do some doctors have a thiriving practice and others barely struggle. Ill give you a hint- one does dentistry on the patients terms, the other does it on their terms. Ill let you figure out which is which.
Dentistry is hard enough- Don't make it more difficult on yourself unnecessarily by trying to do procedures that you know will just make the whole case more difficult. And when its more difficult, its more stressful because the chance of failure is higher.
Sorry for the long rant..... feedback welcome.
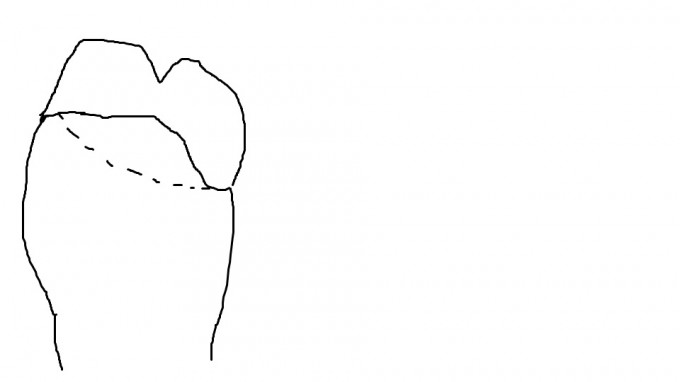
I agree with everything Sam said. My only point was that the case as presented (and we have no x-rays or photos to help) sounds more like a gingival problem (if any) rather than a boney problem. Assuming a need to break the contact on the mesial, any axial reduction can probably flow up on the buccal and lingual towards the distal, as in my poor attempt at art below. In that case the tissue is easy to manage. When you have a lot of enamel to bond too, then dropping margins sub-g when they are not needed will only iatrogenically a create more a difficult situation like Sam describes. Many of our difficulties come because we stay stuck in a conventional crown prep design.
Gary-
I agree with you but I wasnt talking specifcially about this one situation but more in general.
Thanks! One of my colleagues I heard through the 'grapevine' had had problems with at least one Cerec breaking after delivery and I wondered if it wasn't because of not enough occlusal reduction (could have been for some other reason also.)
I think Bob and Ross are spot on. Terrific advice in this thread!
Every restoration has risk of failure, but that risk increases significantly when considerations such as prep design, material selection, bond vs cement, isolation, etc., are ignored or not given due attention.
Thanks! I am trying to 'wrap' my brain around the idea that Cerec doesn't need the same parameters of a prep as we were taught for standard PBM's in dental school (i.e. 2 to 5 degree axial wall taper and 3 mm axial wall height.) Our one Cerec trainer said that he uses a 'plus groove' on the occlusal table and 0 mm axial wall (i.e. level to the gum) at least on some of his preps. I keep this in mind and I always try to engineer into the Cerec prep a little cushion and approach the standard prep because I don't want patients coming back in and saying, "Dr. why is my crown in my hand and not on my tooth?"
There's lots of thoughts on this subject 'flowing through the neurons,' and with significant 'zeal' I'm just going to dive in where I feel is best, with a question first: I feel I have to make the #'s work before I start using milling blocks to make temps and the time it takes and I'm not sure if I am 'immune' in this forum to start throwing out the '#'s' (vis-vis the Sherman Anti-Trust Act) and I guess I haven't used this forum enough to know if that's a 'kocher' discussion so, Can anyone help me with the issue of what can be discussed here as far as maybe regional averages of fees that can be charged for 'Crowns' (I guess that would then cover a temp needing to be milled in the Cerec machine?) Bottom line for me is: Being new at the Cerec crown/ machine processes, I am in the process of working on getting in place protocols and regimes that make the #'s work and gets the patient to the desired goal of optimized oral health and as an office with lots of PPO patients it can be challenging, I think, especially on the front end, to get these patients a treatment plan that works both cost-wise and oral health-wise since a significant # of these patients are to the point of complicated comprehensive oral rehabilitation prosthetics and I want to avoid, 'post-cement problems' with this new technology.
Bouncing off the thoughts above, how about this: Does this Forum feel that its good to charge the patient a separate fee for this 'milled temp crown' (and if so how much?) that the patient would pay for separate from the permanent (PPO) crown, knowing it takes more time to mill (and costs more) than if its out of a kit. Granted as we go forward, we'll get faster and production will benefit too. (I know I'm stepping on some 'raw nerves' in this discussion and I feel there maybe others out there that can benefit from this discussion and what conclusions may come out of it. Thanks!
P.S.1 What the best material to mill the temp out of ?
PS 2 Does anyone out there that's used to doing it the old way have a lab that didn't want to go digital that they feel compelled to use from time to time (well one Cerec mentor said, "Don't think of your Cerec machine as a 'take care of all pt ills' machine.'") (In so many words-that is.)
What do you do about crowns whose margins extend so far apically in the interproximal areas that they violate the 'biologic width' and eventually leave the patient with a concave contour in the coll area so that food/plaque is a continual concern? I don't know about you, but in our office I see many patients whose molars and premolars have severe decay that leaves the restoration in this orientation to the periodontium so its an issue that we've struggled with with our patients even before coming on board with Cerec technology...I have approached one of my periodontists and his comment was, "If the truth be told, many teeth that are crowned in general dentists offices (esp. large buildups and teeth with prior root canal therapy) could benefit from crown lengthening to minimize the above explained gum contour problem." (in so many words.)
Thanks for your thoughts on this issue
Isn't it true that if a permanent crown once fully healed post-op ends up with the marginal gingiva level to the distal marginal ridge (say #31) on the occlusal table that that patient will, when chewing traumitize that marginal gingiva and cause gingival hypertrophy or gingival hyperplasia locally that causes that tissue to become even more thickened which then becomes a food/plaque trap at least in some cases. (I'm not sure and I certainly don't profess to be a periodontist...I'm just thinking about some cases I've seen that came in on recall in the recent past.) Thanks!
On 8/31/2015 at 8:29 am, Dr. Calvin Riley said...Isn't it true that if a permanent crown once fully healed post-op ends up with the marginal gingiva level to the distal marginal ridge (say #31) on the occlusal table that that patient will, when chewing traumitize that marginal gingiva and cause gingival hypertrophy or gingival hyperplasia locally that causes that tissue to become even more thickened which then becomes a food/plaque trap at least in some cases. (I'm not sure and I certainly don't profess to be a periodontist...I'm just thinking about some cases I've seen that came in on recall in the recent past.) Thanks!
I rarely see that. I see tons of patients in their 50's and older with high tissue that has never caused any problems. Most people actually chew with their main mass of food more over the 1st molar-2nd bicuspid area. If it does become a problem it is generally easily rectified with a distal wedge procedure, not boney crown lengthening.
On 8/31/2015 at 8:05 am, Dr. Calvin Riley said...There's lots of thoughts on this subject 'flowing through the neurons,' and with significant 'zeal' I'm just going to dive in where I feel is best, with a question first: I feel I have to make the #'s work before I start using milling blocks to make temps and the time it takes and I'm not sure if I am 'immune' in this forum to start throwing out the '#'s' (vis-vis the Sherman Anti-Trust Act) and I guess I haven't used this forum enough to know if that's a 'kocher' discussion so, Can anyone help me with the issue of what can be discussed here as far as maybe regional averages of fees that can be charged for 'Crowns' (I guess that would then cover a temp needing to be milled in the Cerec machine?) Bottom line for me is: Being new at the Cerec crown/ machine processes, I am in the process of working on getting in place protocols and regimes that make the #'s work and gets the patient to the desired goal of optimized oral health and as an office with lots of PPO patients it can be challenging, I think, especially on the front end, to get these patients a treatment plan that works both cost-wise and oral health-wise since a significant # of these patients are to the point of complicated comprehensive oral rehabilitation prosthetics and I want to avoid, 'post-cement problems' with this new technology.
Bouncing off the thoughts above, how about this: Does this Forum feel that its good to charge the patient a separate fee for this 'milled temp crown' (and if so how much?) that the patient would pay for separate from the permanent (PPO) crown, knowing it takes more time to mill (and costs more) than if its out of a kit. Granted as we go forward, we'll get faster and production will benefit too. (I know I'm stepping on some 'raw nerves' in this discussion and I feel there maybe others out there that can benefit from this discussion and what conclusions may come out of it. Thanks!
P.S.1 What the best material to mill the temp out of ?
PS 2 Does anyone out there that's used to doing it the old way have a lab that didn't want to go digital that they feel compelled to use from time to time (well one Cerec mentor said, "Don't think of your Cerec machine as a 'take care of all pt ills' machine.'") (In so many words-that is.)
Whether a temp is milled or not makes no difference to me. The only time I would charge a separate temp fee is for long-term provisionals such as when testing out opening the bite, and they need to be in place for an extended period of time. Routine temps are part of the procedure. If I mill it, my assistant and I are free to do some other procedure on that or a different patient, The cost of the block is a wash with the time and materials to hand make a temp, so I would not agree with your assumption that the milled temp costs more, especially given that you can do other procedures during the milling process.
I don't feel "compelled" to use any perticular lab. There are lots of great labs that will accept digital files. I am all for loyalty, but if your lab is not willing to grow with you then IMO it is appropriate to re-think the relationship.
Thanks for your reply...just want to make sure though...what are you saying is ideal treatment given the info included here? If patient says 'No' to ideal treatment then what's the alternative treatment plan? Again with the info stated here? Thanks!
I guess I'm not well versed in the process of temporization w/ Cerec milled temps. The type of material in the block, the type of cement that can hold the temp on but not be tedious to remove. Any thoughts on this? Thanks!

On 8/6/2015 at 5:12 pm, Gary Templeman said...I agree with everything Sam said. My only point was that the case as presented (and we have no x-rays or photos to help) sounds more like a gingival problem (if any) rather than a boney problem. Assuming a need to break the contact on the mesial, any axial reduction can probably flow up on the buccal and lingual towards the distal, as in my poor attempt at art below. In that case the tissue is easy to manage. When you have a lot of enamel to bond too, then dropping margins sub-g when they are not needed will only iatrogenically a create more a difficult situation like Sam describes. Many of our difficulties come because we stay stuck in a conventional crown prep design.
Gary, I agree with this and here is a case where I have a tooth that is most distal in the arch and the gim tissue is about up to the marginal ridge. maybe 1mm below it. I do the same thing every time when I prep. I use a 2.0 meisinger reduction bur first and see if I need to remove any tissue. in this case I used a diode before doing any more rep to cauterize the tissue and remove it so I could get more of a prep. I was actually able to get plenty of conventional prep form into this.

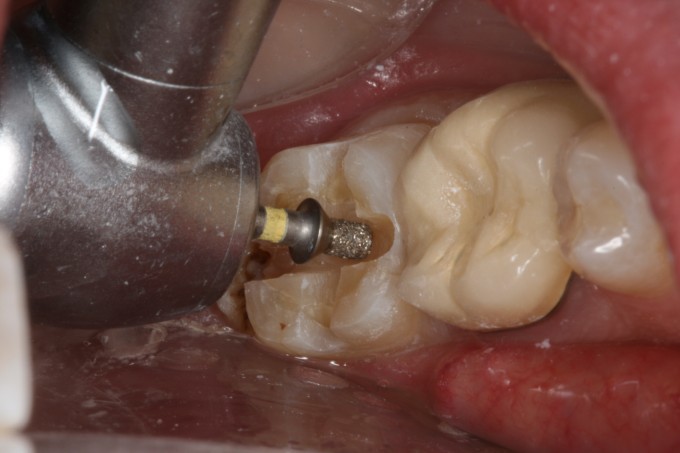

 Notice how much enamel I have because I'm still pretty much at the height of contour of this tooth on the distal. I just need to get tissue out of there and a laser is perfect for this application. You can also use an electrosurge or a ceramic tissue trimming bur. once I do the depth cuts and take off uniformly 2mm, I will use the laser to make sure that my bur does not start any unnecessary heme.
Notice how much enamel I have because I'm still pretty much at the height of contour of this tooth on the distal. I just need to get tissue out of there and a laser is perfect for this application. You can also use an electrosurge or a ceramic tissue trimming bur. once I do the depth cuts and take off uniformly 2mm, I will use the laser to make sure that my bur does not start any unnecessary heme.  once I've done this I keep the margins supra g where I can and sub g where they need to be. hope this helps
once I've done this I keep the margins supra g where I can and sub g where they need to be. hope this helps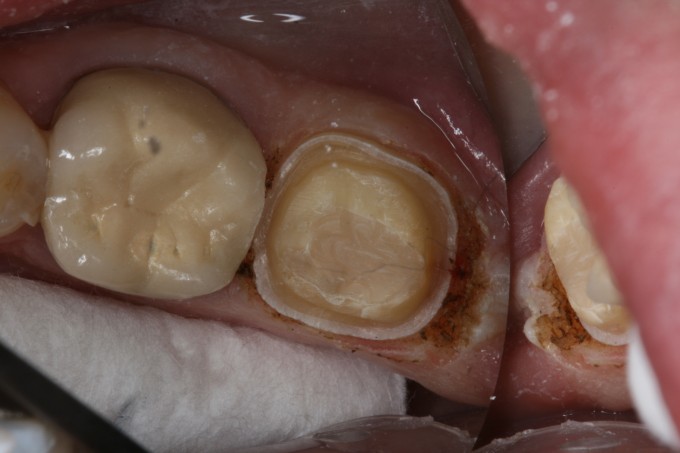

I'm sorry richard, i can't remember what you wrote on account of drooling over that prep. So nice and crisp man, superb

On 8/31/2015 at 9:05 am, Gary Templeman said...On 8/31/2015 at 8:05 am, Dr. Calvin Riley said...There's lots of thoughts on this subject 'flowing through the neurons,' and with significant 'zeal' I'm just going to dive in where I feel is best, with a question first: I feel I have to make the #'s work before I start using milling blocks to make temps and the time it takes and I'm not sure if I am 'immune' in this forum to start throwing out the '#'s' (vis-vis the Sherman Anti-Trust Act) and I guess I haven't used this forum enough to know if that's a 'kocher' discussion so, Can anyone help me with the issue of what can be discussed here as far as maybe regional averages of fees that can be charged for 'Crowns' (I guess that would then cover a temp needing to be milled in the Cerec machine?) Bottom line for me is: Being new at the Cerec crown/ machine processes, I am in the process of working on getting in place protocols and regimes that make the #'s work and gets the patient to the desired goal of optimized oral health and as an office with lots of PPO patients it can be challenging, I think, especially on the front end, to get these patients a treatment plan that works both cost-wise and oral health-wise since a significant # of these patients are to the point of complicated comprehensive oral rehabilitation prosthetics and I want to avoid, 'post-cement problems' with this new technology.
Bouncing off the thoughts above, how about this: Does this Forum feel that its good to charge the patient a separate fee for this 'milled temp crown' (and if so how much?) that the patient would pay for separate from the permanent (PPO) crown, knowing it takes more time to mill (and costs more) than if its out of a kit. Granted as we go forward, we'll get faster and production will benefit too. (I know I'm stepping on some 'raw nerves' in this discussion and I feel there maybe others out there that can benefit from this discussion and what conclusions may come out of it. Thanks!
P.S.1 What the best material to mill the temp out of ?
PS 2 Does anyone out there that's used to doing it the old way have a lab that didn't want to go digital that they feel compelled to use from time to time (well one Cerec mentor said, "Don't think of your Cerec machine as a 'take care of all pt ills' machine.'") (In so many words-that is.)
Whether a temp is milled or not makes no difference to me. The only time I would charge a separate temp fee is for long-term provisionals such as when testing out opening the bite, and they need to be in place for an extended period of time. Routine temps are part of the procedure. If I mill it, my assistant and I are free to do some other procedure on that or a different patient, The cost of the block is a wash with the time and materials to hand make a temp, so I would not agree with your assumption that the milled temp costs more, especially given that you can do other procedures during the milling process.
I don't feel "compelled" to use any perticular lab. There are lots of great labs that will accept digital files. I am all for loyalty, but if your lab is not willing to grow with you then IMO it is appropriate to re-think the relationship.
Great info here, and good questions. Spot on Bob, Ross and Sam (get used to it- they're overachievers)
Agree with Gary on temps- no charge unless for esthetic cases, long term provisionals, or opening up VD in reconstruction cases. Any temp material can work, I like the cad-temp multi because it can mill with the 20s burs, and seems to clog less (hence less time). If you get the carbide burs, this is not an issue. You can also use any of the hypbrids with the normal 20s burs-- this is good if you are trying to keep your inventory down, but as you build, just keep adding to have lots of options in stock. We used to use pvs in a triple tray for temp fabrication, so the cost of the block is really a wash. Also, temping provisional crown with a non-retentive CEREC prep can be an issue. If you have minimal retention on a kind of conventional prep, Durelon is better than most soft temp cements, and cleans off reasonably well--- it chips off in clean big chunks. You could also spot etch with self etching system with flowable, but realistically, if you're sending to the lab, you are going to likely change your prep design.
Good advice to going all digital, and you'll almost certainly find that as your paradigm and philosophy evolves, that the lab case is VERY much the exception.
Looking at numbers is good, but your biggest cost is the fixed cost of the CEREC, and then not using it. The blocks etc are a trade off of other consumable, as well as time, additional appointment, labor etc (these are all big- labor is also your biggest cost in any practice).
One thing to think about, is crown lengthening for restorative reasons is going to be done much less with the principles and techniques utilized in adhesive restorations, and less morbidity for the patient. If it is for biologin width issues, that is another matter, and relates indirectly to the type of restoration you choose to place, and the requirements therein.
Hope that helps...
On 8/31/2015 at 11:23 am, jos dijkstra said...I'm sorry richard, i can't remember what you wrote on account of drooling over that prep. So nice and crisp man, superb
Thanks jos. Def call me Rich. When people call me Richard I feel like I'm about to get in trouble!
The prep is a manifestation of a few things:
1)having a cerec for 12 years and seeing my preps up close and personal for that long
2) caring about what those preps look like and trying to make them the best I can each time (they don't always look like that but at least I try to make them look like that!)
3) being on this site every day pretty much since its inception and seeing so many great clinicians and tips they have shared through the years. I have used what I learned and created a system that I use to prep every time so it becomes repetative and therefore predictable.
Systems and repetition is what makes me efficient using cerec. This is pretty much what I'll be talking about at C30 and how to go from anesthestic to cementation and share the recipe I have used in various steps of the cerec procedure to make you more efficient during that appointment.
