
CEREC TiBase Marginal Accuracy

First time TiBase users often question the marginal accuracy of the TiBase and final restoration in deep soft tissue. The great thing about this system IS the accuracy. The Scanbody, when fully seated on the TiBase or Scanpost, allows the software to propose your final restoration intimately to the TiBase. This intimate connection, bonded outside of the mouth, allows for healthy soft tissue response with both shallow and deeper soft tissue collars. The patient below presented for her final restoration 14 weeks post op implant placement (#19) with 4mm of soft tissue collar after removal of healing cap.
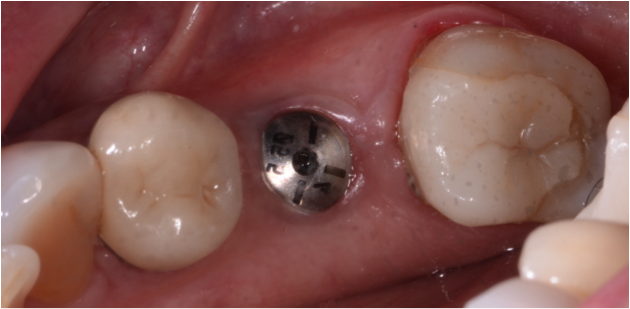
The TiBase and Scanbody were placed and full seat was determined by radiograph.


The crown was designed single unit (un-split) screw retrievable, using the CEREC Chairside software and milled out of an e.max abutment block. Always verify fit of crown (or abutment) to TiBase prior to firing.


After stain and glaze, the final restoration was bonded to the TiBase using Multilink Hybrid Abutment cement and torqued to manufacturers recommendations. Access opening was closed with composite and a periapical radiograph was taken to determine full seat of TiBase to implant platform.


The TiBase to implant complex is the perfect solution in a deep sulcus implant restoration. The crown/ TiBase fit can be visually verified and when bonded outside of the mouth removes the concern of cement clean up and cement sepsis. Note the marginal integrity and fit to the implant platform. When used properly and with proper training on the components and software, the marginal integrity of this complex is no longer a concern.

and what kind of epitelial union is there with disilicate....there is a lot on metal and feldespatic surfaces....but what is happening at those 4mm between the tisular epitelium and the disilicate surface......do you have any studies on that yet ?????
great question...I have no studies or source to determine the attachment histology. Give me a day or two and I will get that. This procedure is so new that we are in the early forms of research and study. Especially at the histologic level. I will talk to a periodontist that will know and answer the question on the Boards.

Dave, Do you place a larger healing abutment to insure that you can fully seat the tibase and scanbody? I don't place implants but I have started to ask the oral surgeon to place bigger healing abutments to try and avoid this problem. Nice case. Thank you for sharing it. See you at study club on the 18th.
Scott, the answer is sometimes. If I can, yes. In most cases I will place a surgical cover screw and primarily close. Depends on grafting needs and stability. I usually use a releasing incision if I see any tissue binding or impingement at delivery. Simple incision MD slightly lingual to mid crest. Tibase falls right in and tissue heals great around crown. Not my trick though...I stole that one from a course. :)
