
 Darin O'Bryan, D.D.S.
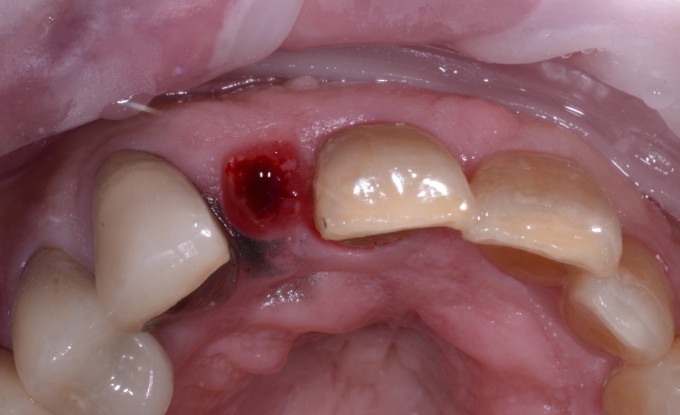
Darin O'Bryan, D.D.S. This case is the classic example of when we get the call from a patient that their crown came off. That call can be anything from a quick recement to this

Needless to say there was not a lot that we could do with this case. So we talked about immediate extraction and implant. Now the trouble is of course getting the tooth out without causing damage to the buccal plate. For this I use the Benex Extractor system. The system allows you to extract the tooth atraumatically to preserve the buccal plate. First you drill down into the tooth. In this case there was not a root canal treatment to follow so I just bored into the root itself.

Once you have a guide path you then place in the engager. This gets screwed in by hand to the proper depth. There are various lengths and widths of engagers with cooresponding drills. The engager has a notch for a cable to be introduced. This cable is then attached to a wench type set up that has a pad for the teeth. The pad rests on the teeth to protect them from the pressue applied when turning the handle to remove the tooth.

The handle on the wench is turned to apply a steady upward force along the long axis of the tooth. The diagram below shows the whole apparatus being used.
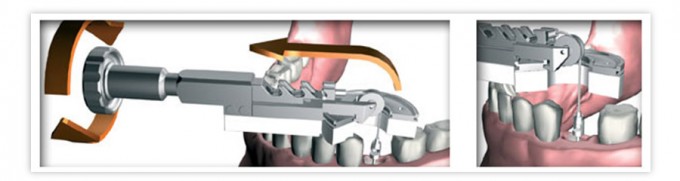
The handle is turned and then you pause for a few seconds. This is repeated until you hear a pop and the tooth comes out.

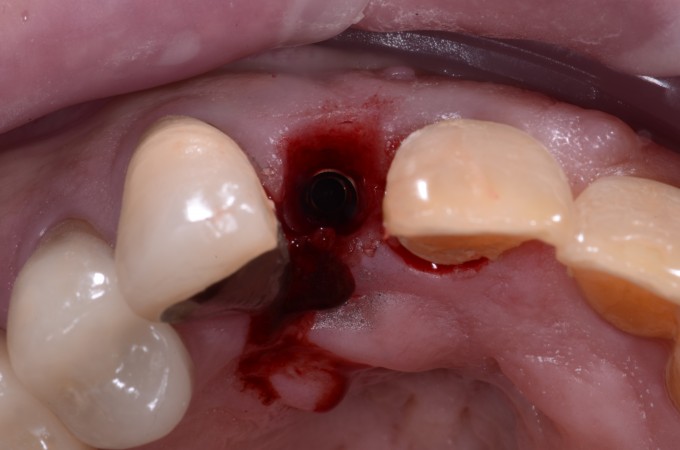
After I got the tooth out I then placed the implant. It was a 3.3 straumann bone level implant. Now if we have a teliocad abutment and tibase we can make a temporary right away. Since these are not out right now we needed another options. Since I had clearance I went with a maryland bridge. This is also a good option when you have to graft or don't get good primary stability. When you do the maryland bridge place either a very short healing cap or in this case the implant was only 2-3mm below the gingival crest. So I placed a cover screw and then created an ovate pontic that almost touched it. There was about .5-.75 mm of distance from the bottom of the pontic to the cover screw.

By creating an ovate pontic I can start training the tissue right from the day of surgery. You can even measure the distance to the contacts to make sure you have 5mm. In this case the patient already has punched out papillae so getting a nice tall papillae probably won't happen. Here is the healed site after healing and integration.


Once we remove the maryland bridge a little bit of lasering is done with a diode to uncover the implant and we scan the area for either the permanent crown or a temporary to train the tissue more if better esthetics can be achieved. No in this case we profiled the bone after healing to get room for the tibase. 
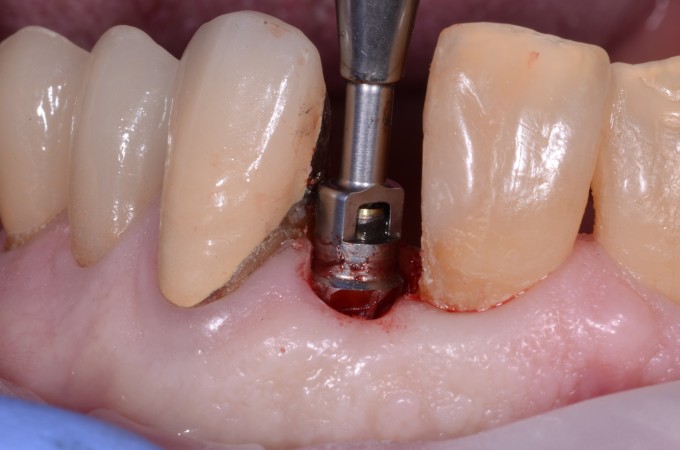
The area is now ready for restoring or training the tissue.
