
Why do guided surgery?




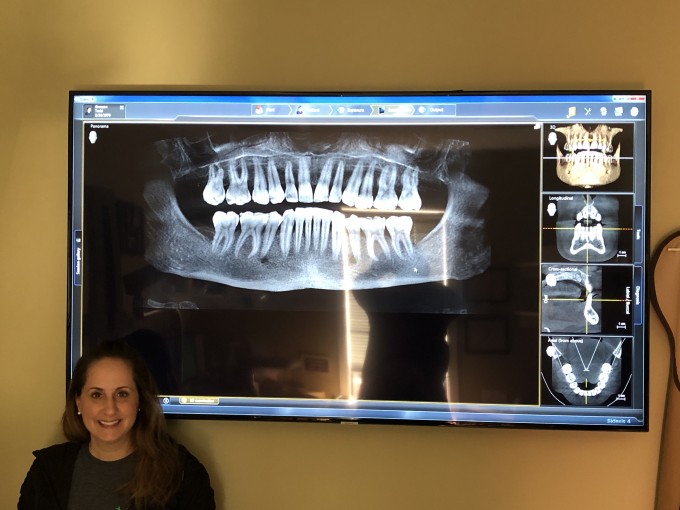
A friend of mine was referred this case by her surgeon. I was really hoping the bite was off but it was verified. My suggestion was to bury the implant on #2 and just restore #3. This stuff makes me so sad and now she has to tell the patient that one of the implants was a waste of money... Rough day for both patient and restoring doctor.

Kris, did your friend have any chance to participate in the helping with the position of these or did the patient just show up? Thanks
On 5/9/2019 at 3:35 pm, Mark Fleming said...Kris, did your friend have any chance to participate in the helping with the position of these or did the patient just show up? Thanks
Patient showed up. It was a referral to her. The surgeon placed them without a restoring doctor in place.

The lack of occlusal clearance between the arches was clearly not part of the decision process or treatment planning in this case. VDO should have been opened requiring more of comprehensive approach, eg: ortho, full mouth rehab. the best that can be done without changing the vertical is screw retained crowns at this point. Amazing to see that implants are still being placed in this manner with all the current emphasis on digital planning.
I have received a number of these "back" referrals in the past. The patient was "talked into" the implants by the implant placement doctor who doesn't restore implants so they show up at our offices. I've refused to treat a number of them because I felt if I didn't do so, I would also be a party to blame for the poor placement. I know the "surgeons" had good intentions but failed to consider the restorative consequences especially in the anterior regions. I guess that's why they have angled abutments and angulated screw channel abutments too.


This has very little to do with guided surgery or lack thereof. The implant angles can be easily restored from what I see.
As Fred mentioned it has everything to do with having the patient bite down and opening your eyes before drilling holes.
Farhad
Good point Farhad. If there was enough room to place the implants it could have been restored with a screw retained crown on #3 and a split crown on #2 or split crowns on both. My point with guided was if it was scanned and planned this would have been avoided because the space discrepancy would have been noticed hopefully. Guided to me is crown down. I am spoiled that way ![]()

Kristine-
Definitely a problematic case. Regarding the restorations, I think that you may be able to do both as screw retained with some careful design. Just plan on seating the distal restoration first, then the mesial. Design the contact between the two such that it allows the mesial one to seat. May take some time in the design, but I think it could be done. It would be nice for you not to have to clean cement from around the distal crown. ![]()
Jay

To say what I really think:
First I must say that I do not do guided surgery. So far I could restore every single implant that I have placed and also not lost one of them.
Only a few implant restorations that I did were ugly, all of them with Cerec. But only once in a noticable way. What are the issues?
When I use angled and comparably small stock abutments (my implant system offers angulation up to 38°) or Atlantis I can restore even unpleasant situations successfully.
The problem starts when I decide to use a tiBase: minimal thickness issues of abutment and veneering structure, very little angulations possible if the position of the implant is not as perfect as possible.
Without the use of a tiBase I often can save any augmentation and also guided surgery because all the discrepancies can be compensated. Sure, it is possible to do it the hard, tiBase way (i.e. augmentation, guided surgery) and it is my work that I get paid for if I do that.
So far I did not choose to invest into a CBCT. (I do a crane CT at a nearby radiologist’s office, of course no Cerec compatibility.) They are awfully expensive and in Germany you can only get about € 130 per scan and the patient usually has to pay it privately. So the ROI is very bad. I think now to have Ernie completely on my side.

Tough case to take over! Really the benefit of guided surgery would have been the "mere" formality of the restorative driven plan, which would have taken the blinders off to a severely compromised occlusion, and a VERY clear problem this side of several thousand dollars, surgery, and frustration.... good luck. Tough case to become involved in the middle...![]()
Mark

Research indicates that about 35-40% of implants have peri implantitis at 10 years. A major factor is often the restoration, cement left behind for sure, but often compromised by the position of the implant (poor contours, cleansability issues, lack of biologic width/space). So even if you have been doing unguided surgery, like many of us, and it appears to be working, many of these implants will develop problems lover time. Guided surgery gives us the best long term prognosis for implant stability, esthetics, and daily home care because we can control many of the factors that will determine what happens at 10 years. Finally, doing implants without cone beams on every one of them is doing surgery blind folded IMO and probably below the standard of care in the US. Don't want to buy one you better have a mobile truck, another practice (oral surgeopn, etc.) or imaging center where you can get one. Not me saying this but Gordon Christensen.

So this may be a very controversial take on CBCT, but I don’t think you can find a dental governing body or body of research saying CBCT is the standard of care. It’s often anecdotal that CBCT it’s standard of care. Now I’m not saying it’s not a valuable tool but the standard of care is really assessing the patient clinically and regular 2D xrays first using the ALARA rule. If and only if you are not certain of certain parameters then should we order CBCTs. For example if a lower first molar site was deemed to benefit from an implant and agreed by the patient, the ridge should be examined for occlusal restorative clearance (like in this case) and medial distal length. Then it would be wise to feel for the submandibular fossa (to see if there is a significant undercut). A PAN can show the zone of safety with great reliability. So if in those above parameters were determined to be satisfactory for restorative space, no significant sub mandibular fossa undercut, ridge looks to be 8mm wide, zone of safety is maybe 13mm or more. Then we can ascertain even a 4-5 mm implant by 10 mm can go in safely without exposing the patient to unnecessary radiation. But if your argument is to take the CBCT because you want to do a guide then that’s fine. However the CBCT shouldn’t be the first line of screening tool to be used.
So I don’t think it’s unfair for us as a prominent group that maybe has some influence in our dental community going around as a group saying that CBCT is a standard of care. We should really be promoting a higher level of diligence in treatment planning with our patients best interest in mind (which includes ALARA) before sticking titanium screws in their heads.
Anyone have a patient have a couple implants placed and had a few before and after CBCTs taken only to have the patient return a few years later with a diagnosis of “throat cancer” only to ask you if all those xrays could have contributed to his cancer? Now the patient isn’t blaming anyone or trying to hold anyone liable for his diagnosis. But how does one answer that heavy question when it comes up.
As I said: I do not have a CBCT but for many years in any case I have a CT done by a radiologist 300 m from my practice.
My implants have a conical connection, so biological width is very rarely a problem. That an angulation could limit the longevity of an implant is new for me and not my experience so far.
But it is true: some of my implants have peri-implantitis, but not one to a degree that it is endangered.
In my implantation cases ridge widths of 8-10 mm are rather rare. To find the optimal length (CT avoids radiographic distortion) and angulation CT or CBCT are essential for me.
Using the tiBase we have to face angulation and minimal thickness problem. And I feel that all these techniques are just work-around of the shortcomings of the tiBase.
Problem would be solved if could just mill our own abutments in a whole like with Atlantis.
Benson,
You bring up a number of interesting points.
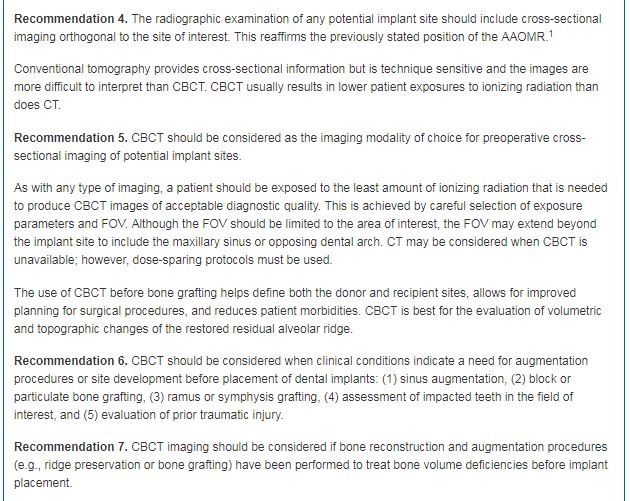
CBCT in many cases is the "standard of care" for implant placement. The AAOMR came out with guidelines on this a number of years ago. It does not establish the standard of care, and neither does any one Association or group. Collectively, the answer is pretty clear. I do a lot of malpractice defense review and testimony, and that changed in our area several years ago.
As far as the submandibular fossa, my fingers do not have the measurement capability to just palpate and know what the 3D anatomy of the undercut is or isn't. I am amazed at the variability of the amount of undercut and angle present in this area. With the lingual nerve and artery close by, this is also a particularly dangerous area.
As far as ALARA, placing an implant with CBCT and a guide results in me almost never needing an intraoperative image, where I usually took at least 2 PAs before.
But I think everyone is missing one of the real benefits from CBCT imaging. I pick up A LOT of otherwise minimally symptomatic or asymptomatic pathology in areas unrelated to the surgical site. In addition, I do a lot of consults for PUO (pain of unknown origin). These patients have often had numerous 2D images without a diagnosis, whereas it shows up clearly on a CBCT. Let's not forget the endo, ortho, perio, and pathology benefits.
One thing to add to Doug’s excellent response: 2D panoramic radiographs do not have the 1:1 anatomic accuracy of a CBCT. You might have magnification errors of 20%, more or less, depending on patient positioning, part of the maxilla or mandible being measured, and type of machine. This matters in that your perceived zone of safety might not be what you think it is. There’s a lot more to this discussion, most of which supports the position of CBCT being used for every surgery, but it’s a bit beyond the scope of this discussion.
J
We all evaluate the risk/reward of every procedure we do. IMO, placing implants without a CBCT can increase risks to the patient significantly for all of the reasons above over 2D imaging. Doesn't mean most of the implants will fail, etc. but with CBCT you go into the surgery with a much higher level of confidence about the best location for any implant. Guided surgery only increases that. Clinical judgement is what this is all about, and in the US malpractice lawyers are being coached to find failed implant cases as a high possible judgement and if no CBCT their chances of winning go way up.

A friend of mine told me about a course she saw in a conference center entitled, "How to make a Million Dollars with Dental Implants." Interestingly enough, the course was not for dental professionals, but for lawyers.
God Bless
matt
On 5/13/2019 at 9:00 am, Matthew Bauer said...A friend of mine told me about a course she saw in a conference center entitled, "How to make a Million Dollars with Dental Implants." Interestingly enough, the course was not for dental professionals, but for lawyers.
God Bless
matt
![]()
![]()
This is one of the funniest posts that I ever read here.
I had an attorney patient tell me once about a course he saw for them called something like “Dentistry and Dental Implants: the Untapped Resource”

Well, Kristine, you opened up a can of worms! Of course guided is the way to go. But the main issue here isn't that so much as it is the lack of the surgeon just putting a mirror into the mouth first and looking at available vertical. And btw, I've never seen or heard that "guided isn't necessary" from anyone who has the facilities for it.
I think I should have chose a different title for this post... my initial reaction when I saw this case was that it was obvious there wasn't enough room to restore a second molar implant. It truly wasn't about guided or not. That was my mistake. My point was more that if it was guided with our workflow of crown down technique then it would have been more obvious there wasn't enough room for that second implant restoration. The periodontist I work with the most rarely uses guides, but we sit down and treatment plan together and he understands exactly what I am looking for in and he can tell me what to expect with any challenges on the case. He does gorgeous surgeries as do a lot of members on this forum- with and without guides. I did not mean any disrespect to that. This was pure frustration for my friend who was at a loss on how to restore this case.
Title edit- "What to do when there isn't enough room to restore and implant".


On 5/9/2019 at 7:03 pm, Farhad Boltchi said...This has very little to do with guided surgery or lack thereof. The implant angles can be easily restored from what I see.
As Fred mentioned it has everything to do with having the patient bite down and opening your eyes before drilling holes.
Farhad
With all the in-depth replies about CBCTs etc (which was excellent), I really love Farhad’s reply. Sometimes we start to run before we walk. Basic preoperative assessment is missed at times, and this is where we end up.
Dan B just posted a nice preop assessment showing the planning for a max cuspid that was in cross bite. Different issue, but same in terms of doing a simple but critical preop assessment.
On 5/14/2019 at 7:24 am, Michael Saso said...On 5/9/2019 at 7:03 pm, Farhad Boltchi said...This has very little to do with guided surgery or lack thereof. The implant angles can be easily restored from what I see.
As Fred mentioned it has everything to do with having the patient bite down and opening your eyes before drilling holes.
Farhad
With all the in-depth replies about CBCTs etc (which was excellent), I really love Farhad’s reply. Sometimes we start to run before we walk. Basic preoperative assessment is missed at times, and this is where we end up.
Dan B just posted a nice preop assessment showing the planning for a max cuspid that was in cross bite. Different issue, but same in terms of doing a simple but critical preop assessment.
That is the point isn't it? We are supposed to be DOCTORS and take the time to assess the situation from the basic to the advanced. Just because there is technology, doesn't mean the basics can be skipped over. Fundamentals, fundamentals, fundamentals! The tech can help, as we discussed here: working from the crown down would have shed light on the lack of room between the arches for the restorative solution!
Agree Kris, your new title fits the post much better.
