
They don't all work out

I much prefer to post cases that are a slam dunk and turn out looking beautiful like this pre-op and 4 year post op case....

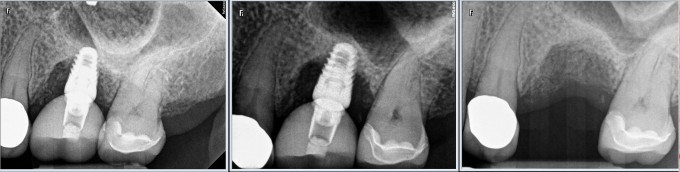
But unfortunately, some cases don't go this way. I hesitated to post this failure, but I tend to learn more from the cases that don't work out. This patient has broken almost every restoration that anyone has placed. She fractured the endodontically treated tooth #14 and I extracted it. I think I only waited 3 months to place the implant.... maybe too soon for this patient. I also went with a shorter implant to avoid sinus grafting.... mistake? Maybe with this case. I let her heal for another 3 months and placed a screw retained e.max/TiBase restoration.
Over the course of about 9 months, things went from bad to worse. I took the crown off, put her in a healing abutment, and grafted, but nothing worked.
So now what? The patient is asking for a bridge, and I'm honestly afraid that she'll fracture the retainer teeth in a few years. Like a lot of you, I offer to re-do everything for free. Right or wrong, she agreed to a new implant, so I changed everything about how I did the last one.
I did a sinus lift, with a bigger, longer implant and re-grafted.

I went with an Atlantis abutment ( I do think a TiBase would have been fine on this case), and I put the softest material I could think of on top, Enamic.

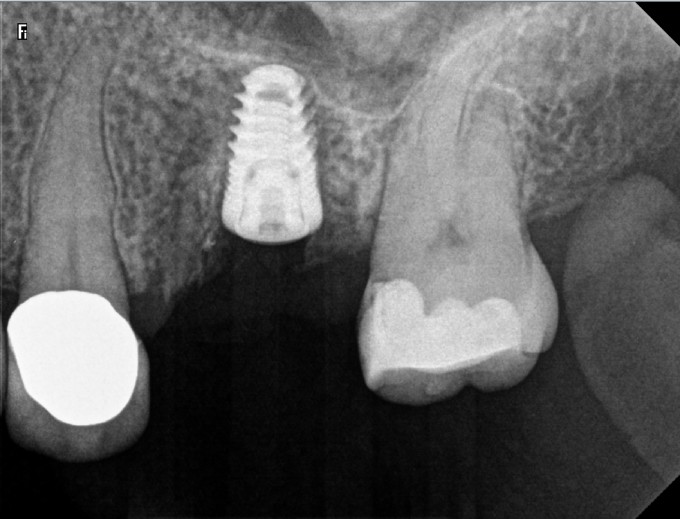
Although I kept the occlusion light, the patient still was functioning heavily on the crown. When she bites hard, I think her natural teeth move apically a lot more than normal.. this is the wear on her Enamic crown after less than a year (delivery and about 11 months).

She appears to be doing well now as far as bone levels around the implant, but time will tell. In the end, I waited longer, grafted more, used a bigger implant, better contour abutment, and softer crown to try and take up some force. Maybe none of this mattered and the case failed for other reasons, but hopefully this is the end of a very long story :)


Great post and thank you for being brave and pointing out the elephant in the room, we all have failures! It is really easy to post all of our most beautiful work, with amazing photography, etc. Those cases inspire me, however, I learn more from seeing how failures are handled. Thanks Dan.

Daniel-
Echoing what Brett said...thanks for posting a less than ideal case.![]() I like your second swing at it strategy. The longer I place Implants, the more conservative I have gotten. I wait four months after socket grafting, and four months after Implant placement before restoring. Even then, I have had the occasional failure. Hope that this case continues to do well.
I like your second swing at it strategy. The longer I place Implants, the more conservative I have gotten. I wait four months after socket grafting, and four months after Implant placement before restoring. Even then, I have had the occasional failure. Hope that this case continues to do well.
Jay

Great Post. We all can learn a tremendous amount from your story. Thank you for showing us a failure.
Kirsten

Thank for sharing. There is a lot to learn from this case. When I'm asked "do you do this or do you do that" it is impossible to answer. The answer should always be "it depends". this case clearly demonstrates this principle!!

I echo the others in thanking you for sharing the case on the board. I think you lost all the grafted bone around the first implant, was it an allograft? That's an awfully agggressive taper, and I've had less than good luck with aggressive tapered implants in allografted bone. With the 2nd implant, I think you got apical stability by inserting through the remaining natural bone which helped to hold the implant in place during function, and the grafted bone is responding to the mechanical challenge like a muscle getting stronger by loading.
Jonathan,
I agree, I did lose all of the grafted bone around the first implant. The graft was a cortico/canc min/demin mix that was placed at the time of extraction. The original implant had a pretty high insertion torque, but it was probably achieved in only a few mm of bone. The implant was fairly well integrated in those few mm, and needed a pretty high reverse torque to remove the implant. I think your assessment is right on, having cortical bone stabilization through the sinus probably helped a lot with the second implant.

I would hardly call that a failure, just a more convuluted success. What type of cement do you use? Why is it that we redo things for free? Are you saying you did not charge for the sinus lift and new abutment? Do orthopedic surgeons not charge for a failed knee replacement? Sorry, I'm kind of crabby today....

Thanks for the post Dan... brings a lot of reality and practicality into the treatment we do, and I think no one bats .1000.... even the gifted (like yourself ![]() ). I'm with you AND Jon----"why do we do it for free?".... we just do... patient relations, a sense of service, guilt, wanting to help, kindness.... all of the above. I respect you for that, and hope your patient does as well...
). I'm with you AND Jon----"why do we do it for free?".... we just do... patient relations, a sense of service, guilt, wanting to help, kindness.... all of the above. I respect you for that, and hope your patient does as well...
Mark

Wonderful post Dan and great rationale for what you did. What implant brand was the first implant?
Farhad
Thanks for all the comments.
Jon, I agree with you in principle about not giving our work away. I think for the reasons that Mark outlined above, it's an easy trap to fall into.
Thank you Farhad, the first implant was an Implant Direct interactive, it's a clone of a Nobel active at the connection. I don't know if the actual implant had anything to do with the failure, but these days I only place Astra EV (that's the new implant here) or Xive if I want a more aggressive thread pattern. Although I've had success with many brands of implants in the past, I just see so many benefits with Astra and Xive and far fewer problems.

Great post Dan! We learn far more from our failures than successes. Thank you for sharing this case
