
"Let's do it blindfolded" she said...
Now that I've got your attention, let me give you some context: I had a resident come through to observe a few months ago, and on seeing the clinical presentation of the proposed site, she felt that there was no need for a guide or even CBCT, and that she could close her eyes and treat this patient.

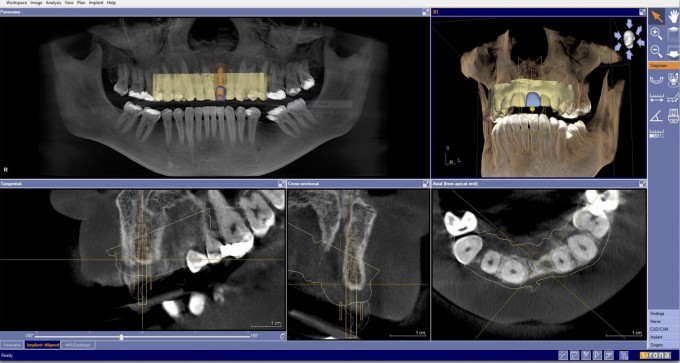
Having followed what is now standard protocol in my practice, I took advantage of the integration of CEREC and the SL, merging the files and creating a prosthetically driven treatment plan. You will note the potential for problems in this surgery due to the very large incisive canal in close proximity to the planned fixture position, hence the surgical guide.
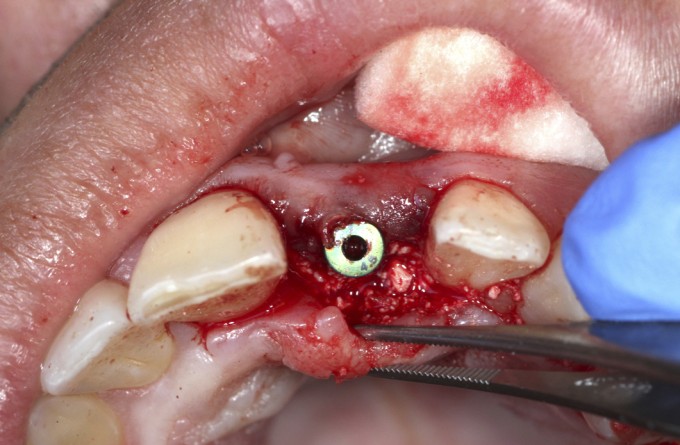
I printed my surgical guide with the Formlabs printer and performed my osteotomy; I have come to expect these guides to be very consistently accurate.


I planned on enucleating the nerve and grafting at time of implant placement, as it was clear from planning that there was inadequate bone on the palatal side for this fixture.
I saw him for his 4 month follow up last week and his healing looks acceptable enough that I am releasing him to his restoring dentist.
I was thinking about this case and the comments of the resident, and I imagined attempting the case without the benefit of three dimensional prosthetically driven planning. I was thinking about how hard it would be to keep my osteotomy true without the benefit of the guide; it would be so easy to end up either too far buccal, or perhaps perforate the palatal and end up in the incisive canal space. I went back and looked at this view again...:
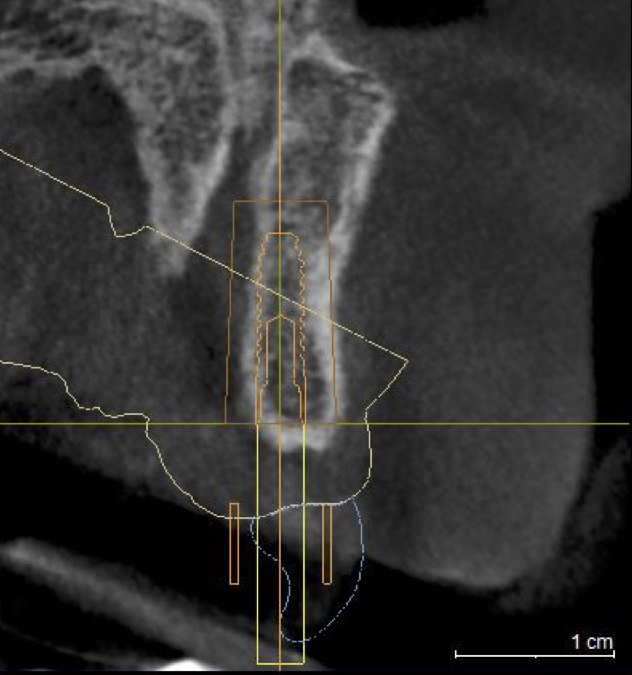
...and it reminded me of why I made the commitment to add this technology to my practice: it increases the quality and consistency of care I can provide for my patients. In hindsight, working without these tools and their protocols is very much like doing it blindfolded, and it is not fun.
Jeremy

You definitely got my attention! I expected the post to be about your #metoo moment. :-)))
Nice case. You are nicer than me. I would have probably enucleated the incisive canal and grafted it at the time of placement (both the canal and the buccal).
Guided makes threading the needle much less stressful!
Thanks David! I'm sorry I didn't relate it well; I did graft the canal at the time of implant placement. The planned position left enough intact facial bone that grafting there would have only served as a contour graft, and that wasn't necessary for this particular patient.
Jeremy

Certainly a well executed case and this will turn out to be a nice result. Just 2 things I personally might have done differently:
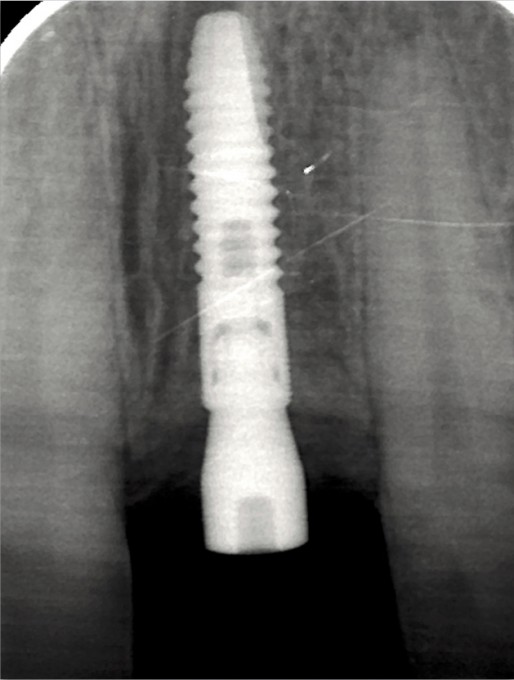
1.) Based on where the implant is emerging restoratively (slightly mesially it looks like) and based on the periapical radiograph it looks like there was room to move the implant distally (and then possibly tilt slightly mesially coronally if needed) to get the implant further away from the canal.
2.) In my hands it would be more predictable to move the implant more facially and then tilt the coronal aspect more palatally to get the implant further away from the canal and then contour graft the facial instead of partially enucleating and grafting the canal through the minimal flap opening.
Farhad
Thank you, Farhad. I recall struggling with that position quite a bit. The canal had an irregular shape and it was very difficult to find a position that compromised only the facial or the lingual. The final position was chosen based on this; it could of course been handled in different ways, but that was my thought process. His palatal tissue was incredibly thick and it took a long time to dissect it out to the point I could visualize everything. I completed the osteotomy first, then enucleated the canal approximately 14mm and grafted it after I placed the fixture; I was able to see, but it was difficult holding that tissue out of the way. I thought several times about releasing more, and second guessed the planned position more than once. As you point out, not the easiest case in more than one aspect, but the suite of technology certainly helped me execute in a way I'm not confident I could have done without!
On 5/8/2018 at 8:22 pm, Jeremy Bewley said...Thanks David! I'm sorry I didn't relate it well; I did graft the canal at the time of implant placement. The planned position left enough intact facial bone that grafting there would have only served as a contour graft, and that wasn't necessary for this particular patient.
Jeremy
I see that now! Sorry for the confusion. I initially thought you were saying that guided allowed you to avoid grafting the canal. Great case!! I know that you are a big biohorizons user... have you switched, or do you use multiple systems depending on the case?

Why chose the 4.8 implant instead of a 4.1 or narrower that would leave more surrounding bone?

Jeremy - quality work as always and such a great learning case to see how other clinicians would approach and execute these types of cases!!
On 5/9/2018 at 6:54 am, Kenneth Magid said... Why chose the 4.8 implant instead of a 4.1 or narrower that would leave more surrounding bone?
This was an Astra EV 3.0x13. The numbers on the healing abutment are 4.5 for height, and 3.5 for diameter.
J
On 5/9/2018 at 6:50 am, David Sullivan said...On 5/8/2018 at 8:22 pm, Jeremy Bewley said...Thanks David! I'm sorry I didn't relate it well; I did graft the canal at the time of implant placement. The planned position left enough intact facial bone that grafting there would have only served as a contour graft, and that wasn't necessary for this particular patient.
Jeremy
I see that now! Sorry for the confusion. I initially thought you were saying that guided allowed you to avoid grafting the canal. Great case!! I know that you are a big biohorizons user... have you switched, or do you use multiple systems depending on the case?
I've used quite a few systems, but Biohorizons has been my preferred system for a number of years. I have added Astra EV to the fold mainly because the prosthetic attachment is superior to that of Biohorizons. The down side of EV is that the threads are less aggressive and it's more technique sensitive to prep the osteotomy and deliver the fixture in soft bone or immediate sites. I'm selecting the best tool for the job, as you suggest
Jeremy
On 5/9/2018 at 7:02 am, Andrew Hall said...Jeremy - quality work as always and such a great learning case to see how other clinicians would approach and execute these types of cases!!
Thanks Andrew; I also like sharing these kinds of cases. It gives people something to think about, and as evidenced by Farhad and David, offer alternative treatments or methods that might be considered.
Jeremy

Jeremy-
Great case!! Very well thought through. I hope that your resident friend has seen the case, and that it was an eye opening experience for her. ![]()
Any concern about using a 3.0mm diameter Implant to replace a central incisor? Have only used these for lateral incisors.
Jay
Thank you Jay
No...the biggest concern for me has been creating an emergence off that platform and managing the soft tissue properly. I thought about using a Biohorizons 3.4 or 3.8 tapered plus, but either of those would have also had a 3.0 platform, and I liked the connection better for this case. Will it make a difference? I don’t know.
Jeremy

Jeremy-
That's a great case- thanks for sharing.
I have never done an enucleation of the palatal canal- Is it simply done by removing it using a curette and filling the space with allograft?
What kind of post-op does it leave for the patient? Are they "numb"in that area afterwards?
Thanks for the education! and maybe you could use a blindfold if you're using a guide.
Hi Brad
I usually use a surgical hand piece and long round aggressive bur (from Salvin, I think). I’ll have to look up the actual part number. Rotary in combination with manual curettage. I believe I mixed PRF into the allograft in this case and used a memlok pericardium membrane as the graft included part of the coronal aspect of the fixture on the palatal side.
Post op discomfort is usually no different than any other open flap procedure. I’ve not had a patient complain of anything, really, although they do have loss of sensation there.
Jeremy
