
Predictable implant restorations: working backwards to move forward

There are very few procedures that are more profitable and efficient than restoring implants. Typically, by the time the implant is ready to restore, the patient is committed to treatment and ready to get their tooth. This usually reduces the number of financial issues and limits no-shows and cancellations. The icing on the cake is if you are restoring with CEREC, you can count on the cost of restoration (whether custom abutment and crown or screw retained restoration) to be considerably less than it ever has been.
But, we all know that ideal world doesn't happen every case. Most of the "complications" I have experienced are due to poor coordination of care with the surgeon, or improperly setting expectations from the patient. I've see where the patient agrees to surgery at a specialty office but forgets about their financial responsibility for the restoration. I've experiences the surgeon including an abutment in the cost of surgery, which means the restorative specialist now is stuck with a stock abutment that the patient has paid for, when in reality we would prefer to use a custom abutment or screw retained restoration.
Even worse than any of these financial barriers that can be raised is when the surgical outcome deviates from ideal, which creates a fundamental dilemma in how to restore the implant. We've all see cases where we have to go through all kinds gymnastics simply to restore the implants.

Wouldn't it be nice to have something predictable and straightforward to design instead?
To predictably set yourself up for this type of straightforward, no-nonsense restoration, properly planning the surgical case from the beginning is an absolute must. The general dentist acts as the quarterback for our patients. We create the plan and then either hand off to another person on our team or throw the touchdown ourselves. Something I see too often in dentistry is the "hands-off referral" where we send the patient on their way with a referral slip and don't even hear anything about the patient until a progress note from the specialist. This is not a good approach in general, but especially when it comes to implant dentistry. Whether we provide the surgical services ourselves, or send the patient to a specialist, we can make our restorative lives better and ensure our patients have a better outcome by planning the case properly before we begin.
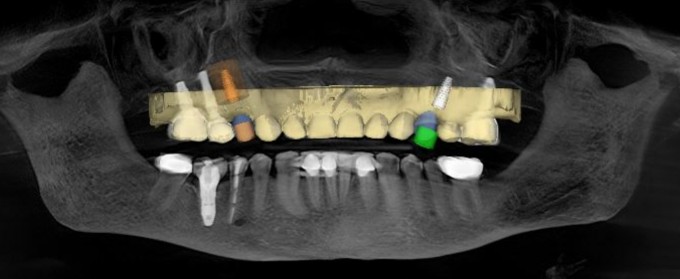
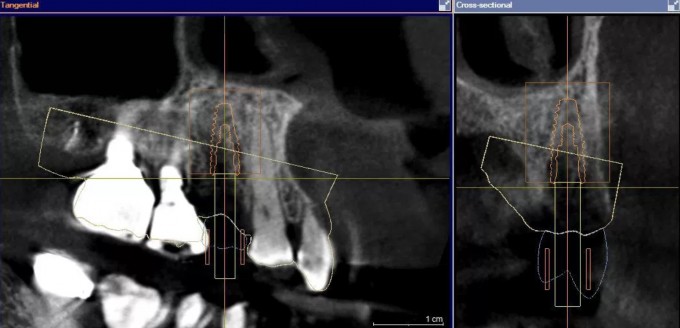
In this case, I planned out the surgical aspect by merging Galileos and CEREC data. The way I plan this out is with the restorative outcome in mind from the beginning. I can account for proper angulation to allow for a screw retained restoration in both the #5 and #12 positions. I also ensure proper depth of placement to allow for the ideal emergence profile. Finally, I made absolutely certain to avoid an anatomic concerns, like the sinus cavity, adjacent teeth and implants, and the thin buccal plate. I then fabricated a surgical guide based on this plan that would allow me to execute exactly as I planned out.
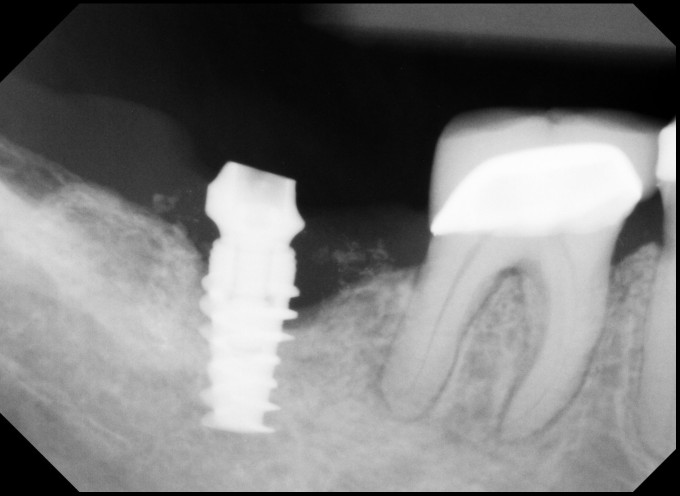
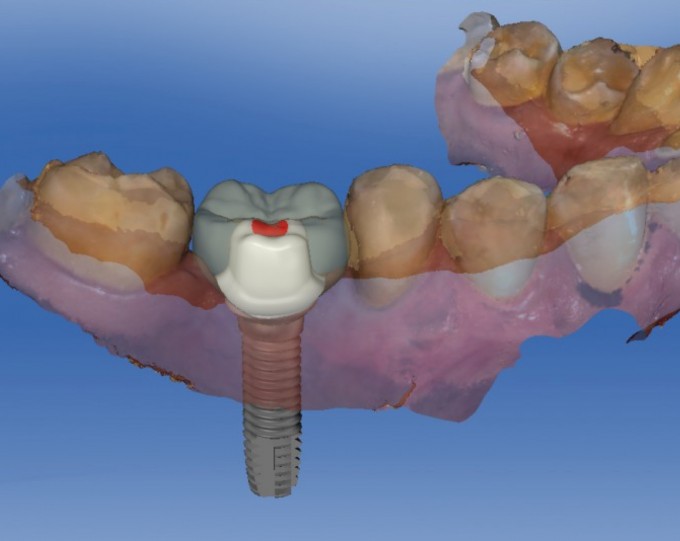
The beauty of all this hard work and planning is when the implants were ready to restore, I knew I would have no trouble at all obtaining great results with proper angulation and depth to allow for ideal screw retained restorations. The restorations were imaged, designed, and fabricated with the CEREC tibase workflow using e.max LT as the final material. Custom shading created the final lifelike touch to the restorations

Sometimes there are cases that need attention from a specialist colleague. Using this workflow and this way of planning out the case allows us to still get to this point from a restorative aspect. And if we plan the case out properly from the beginning, and follow proper guided surgery protocol, we all can see this type of result from all of our implant cases

As always, a homerun JP.
Love the digital workflow that removes the guesswork from these procedures.
