
Thread to post day to day work

At the IDS a couple of us had a conversation about the cases that were being posted to the forum. Over the last few years most of the posts have gravitated towards Anteriors, zirconia and Implantology. While it's understandable that these are new and exciting applications that a lot are learning, I feel that we have gotten away from posting the day to day stuff that all of us do (far more than anteriors and implants). I have also been a part of this only posting interesting things and my best anterior work.
So... The purpose of this thread is 3-fold:
- Posting day to day work. Even if it's not your best stuff. Better yet, maybe some stuff that did not work out very well
- To help all of us learn. While I understand if I post a great case many people will say "good job" or want tips on how to do it... there is less learning than just simple day to day stuff for most on the site.
- Learning to document you cases. There is no better way to learn than forcing yourself to document your cases. I know it's hard and time consuming at first... but you will be better for it!
I will start with a case I did today that was simply exhausting. I just wanted to get done with it...LOL :)
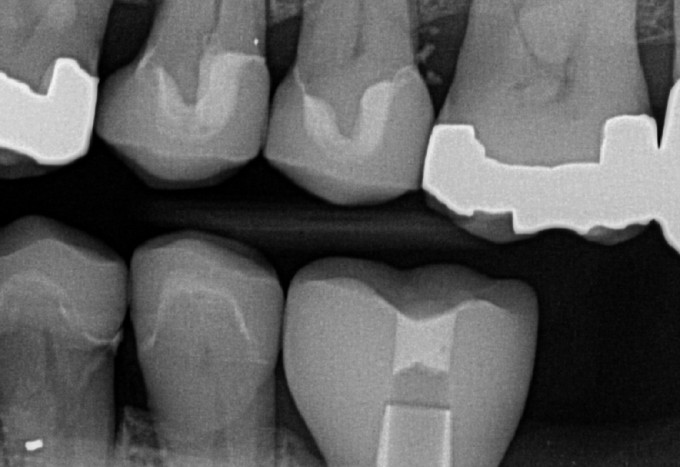
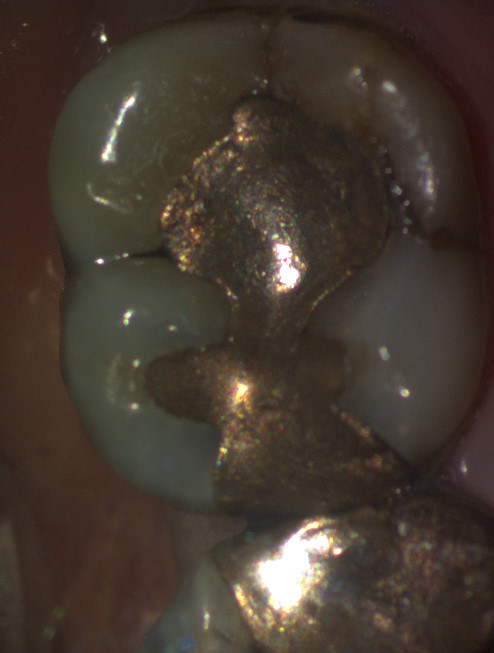
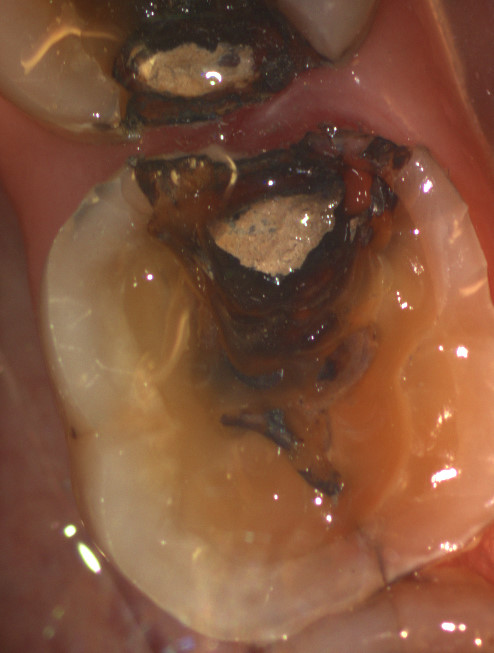
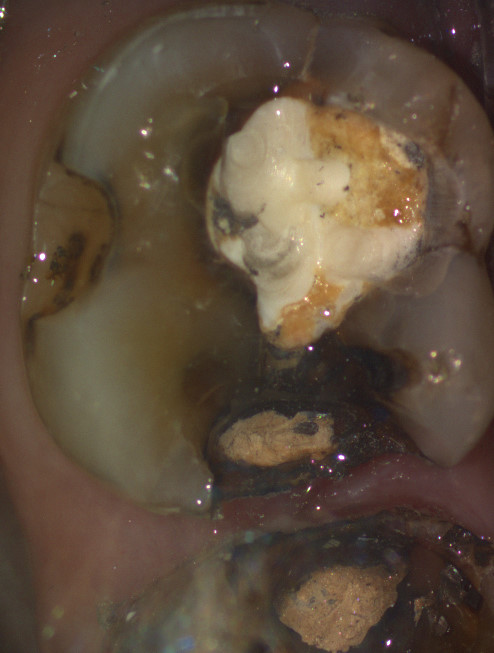
This is a patient I have slowly been restoring over the years (as his budget allows). He has massive defective restorations and decay forming around many. Today I treated 12 and 13.

The first suggestion that I have is to use a rubber dam. Now even though I will not be able to use rubber dam the entire time, I know that I have massive restorations and decay to remove and will also have to do buildups. Having the rubber dam not only makes this easier on you, but also the patient.... who wants to have all of this flying all over their mouth. It also helps isolate when doing the buildups.

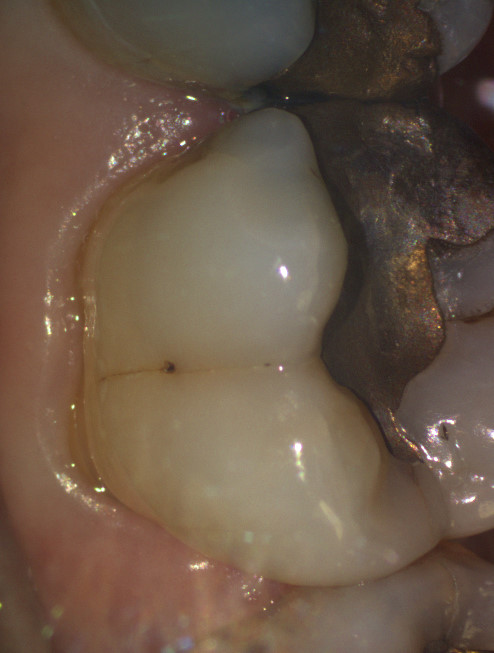
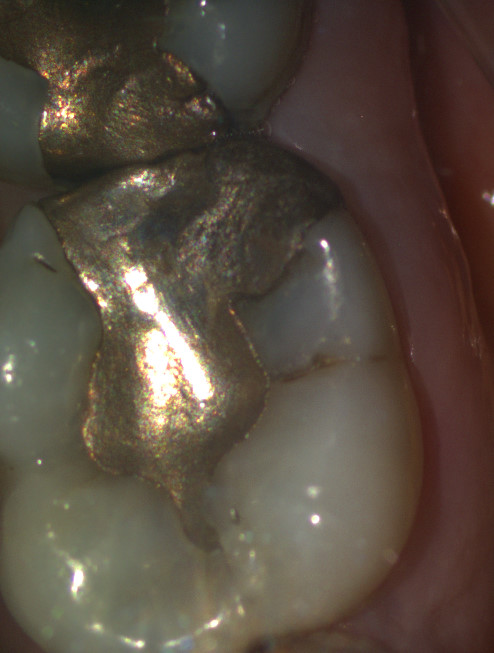
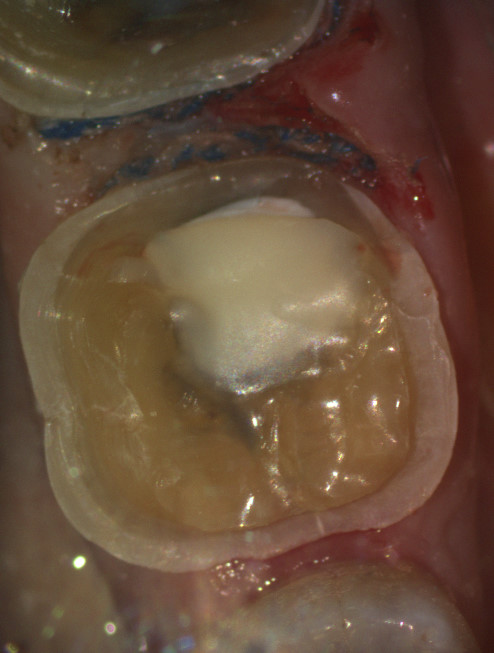
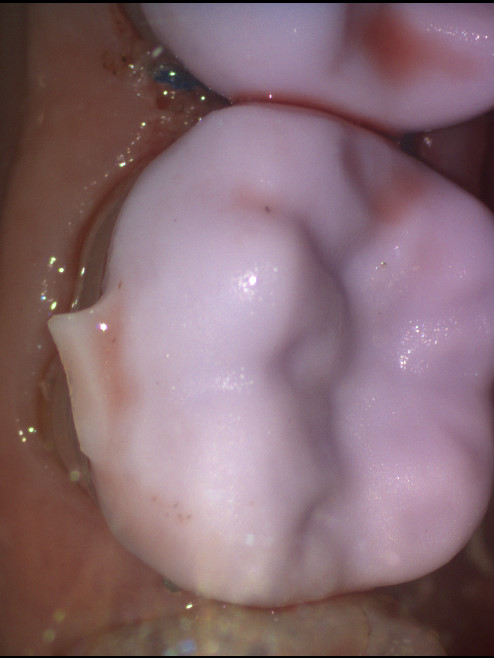
I then removed the rubber dam and finished the preparations. He had a lot of undercuts that I needed to prep out, so I opted for a very long chamfer margin. The margin on the distal of 12 also had a defect, so I decided to leave that margin in composite (margin elevation). I felt comfortable doing this because I has such good isolation when doing the buildup. I also disked and recontoured the adjacent teeth because I know they will need restorations in the future and I wanted the crown contacts to be more ideal. This also will make "picking up the contact" with the Omnicam easier

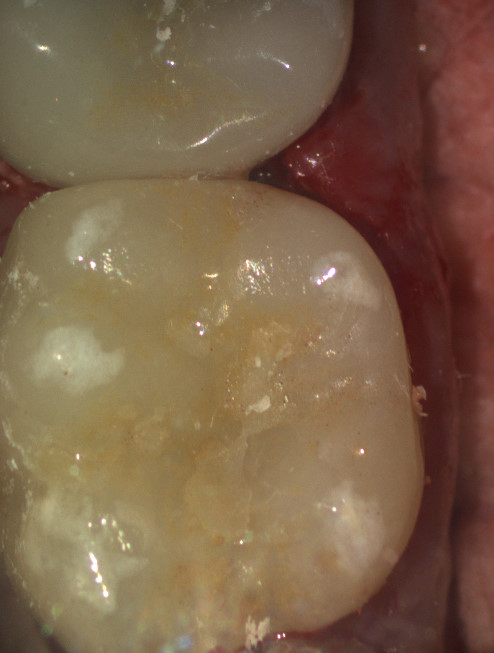
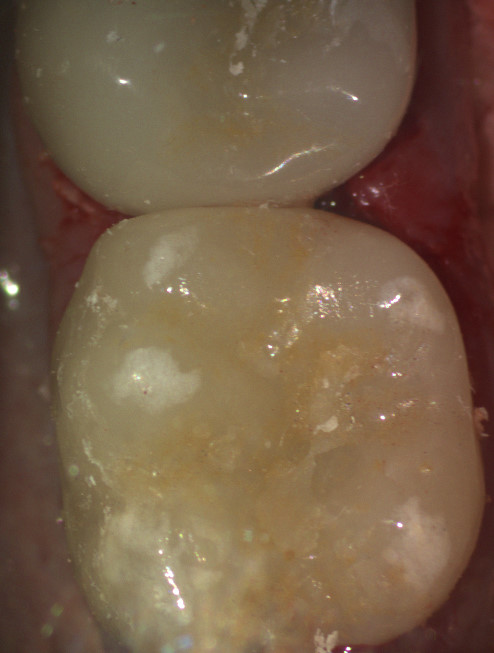
And here are my final restorations. This is just day to day stuff. I was far too exhausted to get overly crazy with the stain and glaze...LOL. It was a long appointment :) They are e.max restorations that were cemented with RMGI. I don't bother anymore trying to bond in a field like this when I cannot get it fully isolated.


I've been using speedcem plus for those kinds of situations Mike; what are your thoughts on that vs a gcem or the like?
J

Even if it's just for practicing documenting. Do it. Absolutely no one will judge you here. Only here to help everyone improve.

Mike #12 concern about possible rct?and wonder do you try to avoid, if no symptoms I try to avoid and explain if rct needed with in two years will redo crown for free and only charge for rct and p&c and not charge for new crown.......what do you do?

On 4/4/2017 at 4:48 pm, Gene Messenger said...Mike #12 concern about possible rct?and wonder do you try to avoid, if no symptoms I try to avoid and explain if rct needed with in two years will redo crown for free and only charge for rct and p&c and not charge for new crown.......what do you do?
Gene, why he has to redo for free?
Patient has high risk of bio and crowns are definetely is the best option in this case. Look at tooth #21, this is enviroment problem not the restoration. Patint has to understand that doctor does everything in his power to be more conservative. Gregory


On 4/4/2017 at 6:36 pm, Farhad Boltchi (Faculty) said...Mike,
Can you please show us how to make Slime?
Farhad
All you need is a little Borax, glue and food coloring. Come on Farhad :)
On 4/4/2017 at 4:48 pm, Gene Messenger said...Mike #12 concern about possible rct?and wonder do you try to avoid, if no symptoms I try to avoid and explain if rct needed with in two years will redo crown for free and only charge for rct and p&c and not charge for new crown.......what do you do?
Hi Gene-
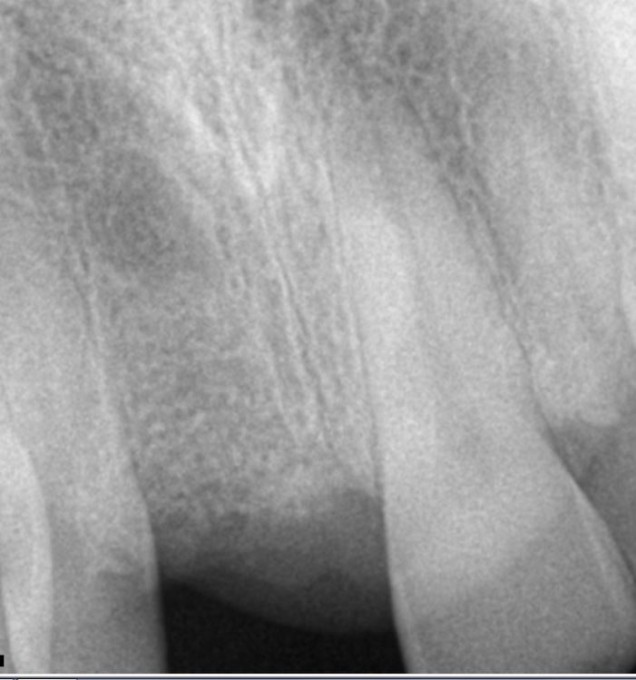
We did talk about it, but he has no symptoms or radiographic pathology... so we will watch it. If it happens, it happens... nothing you can do. What I charge depends on when it happens and to be honest the patient.
Like Gregory pointed out... this patient was a mess when I first met him. The good news is that he is doing better. We wish we could restore everything now, but financially it's not an options. We have been working on him slowly for over 7 years now. I have done an implant on #10 and 19, bridge on 29=31, crowns on 3,4,5,12,13, 20 and 21. In fact... the restoration that Gregory pointed out (#21) was the first one(s) (with #20) that I did a little over 7 years ago.
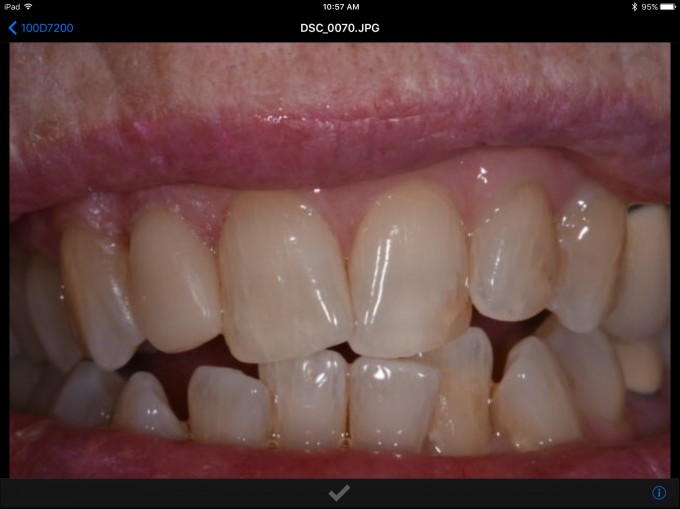
Here is a picture from 2 years ago when I seated that implant restoration on #19 (so #20 and #21 are at 5 years post op here)...You saw the xray from 7 years post op taken today. They are doing great


Thank you for this post!! I have done one crown and I am trying to find time for the first Cerec training. I have been reviewing case presentations and everything I viewed seemed so foreign to my general dentistry practice. Thank you for showing a case similar to what I do and reassuring me I have not made a mistake with this purchase. Now I can go to sleep and not have nightmares. Thank you again.

Great idea for this thread. I think the day to day stuff works so well that we all take it for granted. It's also tough to take the time during a buys day to document cases. My hat goes off to all of those on this board that take time to share them.
I'll support Mike's idea.
This was Empress onlay back from 2009. DL cusp caries and fractured. We can also see bifurcation area involved and I had to reshape my prep to give proper space for gingiva and avoid overhang at bifurcation area as you can see at the prep pictures. I did small gingivectomy with soft tissue laser.
e.max A2LT was at this case. Cemented on Calibra Universal. Gregory








Mike and all
Phasing things is how we do so much. I am glad to see more day to day also. I will post more and will be happy about it!!!

Old case. Bridge repair with emax that is actually still in service. I miss the blue cam and 3.8 software ![]()





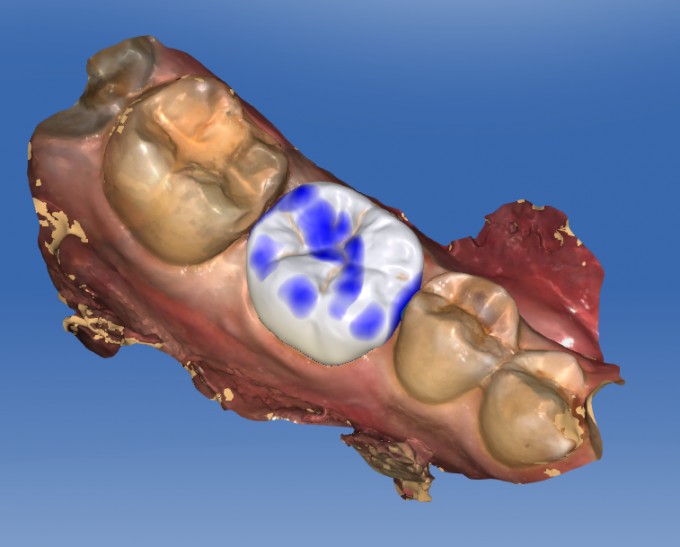
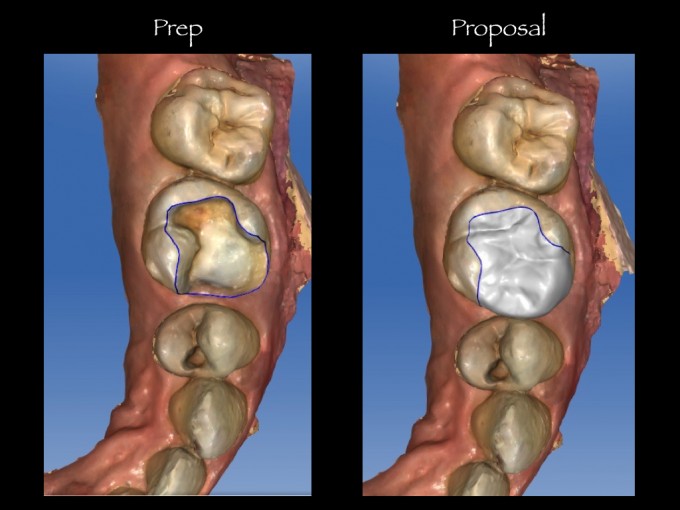
Ok here is my contribution to the thread. Rotated tooth, broken cusp. You know the drill:

Teeth prepped conservatively:

Finished Case:


So here is my contribution to this thread.
Q: What happens when you designate Scan post instead of Tibase for an implant restoration?
A: You get a patient that's 'long in the tooth'
Sorry

Here is mine today. Patient not want tooth as dark as 31 or stains. This is Celtra Duo Polished only Still had little cement clean up to do Photo right after seating set.



On 4/5/2017 at 8:44 am, Kunal Lal said...So here is my contribution to this thread.
Q: What happens when you designate Scan post instead of Tibase for an implant restoration?
A: You get a patient that's 'long in the tooth'
Sorry
That is epic!!

On 4/5/2017 at 12:55 am, Regina Powe said... Thank you for this post!! I have done one crown and I am trying to find time for the first Cerec training. I have been reviewing case presentations and everything I viewed seemed so foreign to my general dentistry practice. Thank you for showing a case similar to what I do and reassuring me I have not made a mistake with this purchase. Now I can go to sleep and not have nightmares. Thank you again.
Regina
Congratulations, you will love this. I spent the first weekend with CEREC practicing on a typodont making crowns over and over. Helps build confidence.

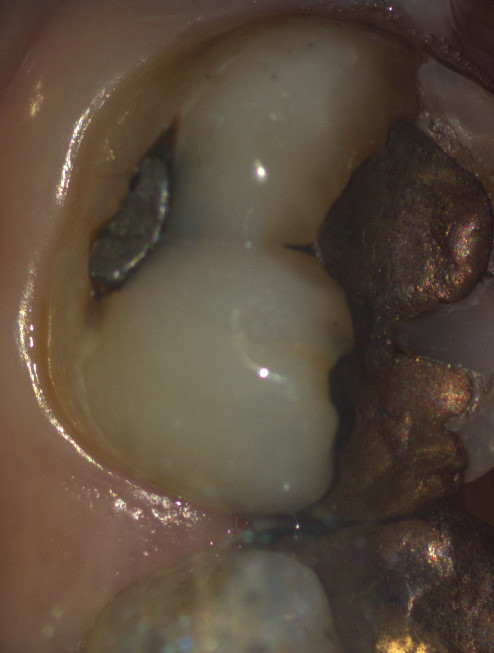
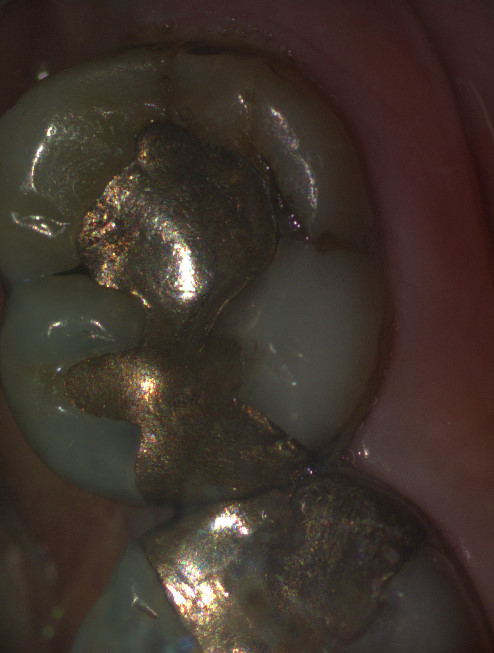
Nothing fancy but here is a partial coverage case on #3. Failing MO amalgam and obvious fracture on the MB cusp. If I have mesial and distal fractures, I tend to favor crownlays or full coverage but for cases I like this, I tend to try to be as conservative as possible. I like GC Cerasmart of 3M Lava Ultimate for my inlay/onlay restorations. It mills out great, polishes nicely and in my experience, I think composite/hybrid blocks do better at the cavosurface margins as compared to ceramics (i.e. e.max/Mark II), and it is repairable with composite if there is some marginal breakdown occlusally. I don't have anything longer than 3 years to give a great long term personal remarks, but so far so good.
Summary of this restoration:
#3-MOB Onlay with GC Cerasmart A2 HT
Selective Etch, Adhese Universal Bond, Variolink Esthetic Warm


On 4/5/2017 at 9:53 am, Thad Vincent said... Nice Celtra Duo! Sam, what materials for your case?
Inlay was Cerasmart. 3/4 crown was emax MT.

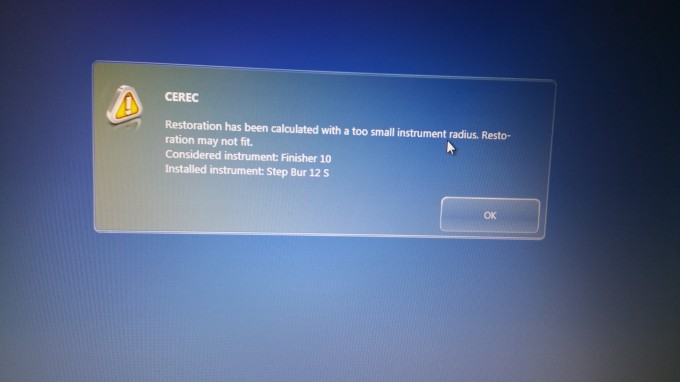
So this message popped up for Zirconia dry mill and I ignored it and surely crown did not seat. In this message it says that consider using finisher 10 which I already had installed and Step 12 bur was also installed as I have four motor unit so do not understand what happened here. If anyone has any thing to say about this to keep in mind for the future. Also since restoration did not seat and it looked I will spend long time adjusting contacts, put him in temp crown and got printed models of scan from Infinident, adjusted my crown on model, glazed it, today patient came in and I still was not able to seat it along the path of the draw, has to go from buccal and mesial contact seems light but not open. Any tips is greatly appreciated for this issue.

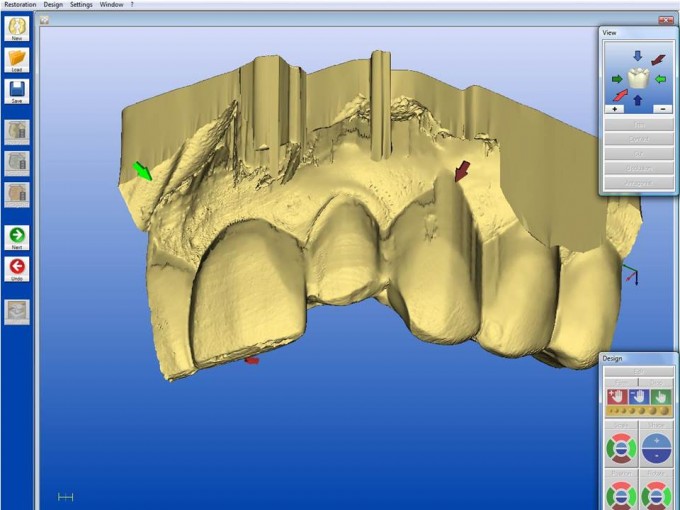
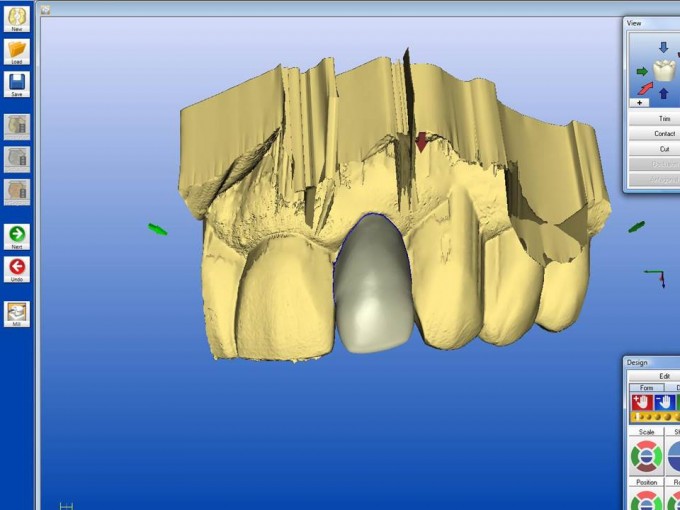
This is some of my day to day work.Nothing unusual except I had to do it myself.My son has been doing all my designs and Cerec work for 5 years and he left for Dental school last week.Seems like my old skills are still there.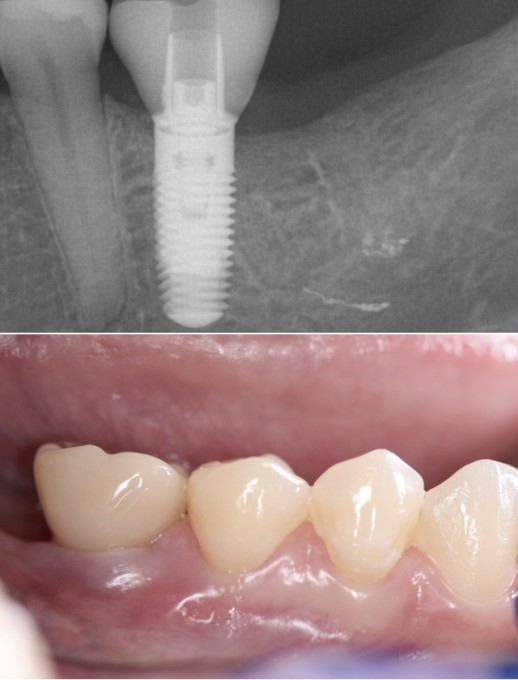
Ashish-
When you got that error, did you start out as emax and then switch it to zirconia? You get that error sometimes since the lumen is calculated different. With way, to fix it, go back to design and change spacer up 10 and hit ok and the back down 10 and hit ok... go back to mill and it's fixed
Here is an interesting failure that I had...This case was initially done in 2012
Preop situation #3:

The tooth was actually asymptomatic at this point, but needed a crown.
At this point (5 years ago), I was still prepping modified flat tops (not completely flat... but very high in enamel). I tend not to prep like this anymore. Here was the way I prepped the tooth:

Now as you can see there is a very prominent crack there. I saw it at the time as well, but the tooth was not symptomatic and decided it was more important to have good enamel.
I restored this with Vita Enamic. It was a new material at the time (we may have even been testing... i don't remember). Here is the lingual view:

The fit was incredible and I was very pleased with the restoration.
Now fast forward to June 28th, 2016.. he came in with this:

Not only did he crack the restoration, but the entire mesial and mesial lingual (right along this crack)....
So, what happened? Well, looking back, I made 2 foolish decisions in this process:
- Wrong preparation with that crack. I should have prepped traditional full coverage crown
- Wrong material. I never should have used Vita Enamic for this case
How did Vita Enamic contribute to this failure?
- I'm not saying that if I used a stiffer, higher modulus material like e.max this would have survived. However, because I used a low modulus material like Enamic, the forces of day to day chewing were transferred directly to the tooth. It's an interesting failure because the bond did not fail because of all the enamel it was bonded to. The reason it failed was because Vita Enamic is a very resilient material... it flexed during mastication and the forces where transferred down and out. Because the crack was there... it cracked the tooth still and took 1/2 of the restoration. If I used e.max, the material itself would have taken more of the force and even though it still likely would have failed because the preparation was wrong... it would have had a better chance.
I restored again with zirconia.


Mike! You are my Sheldon. And I love your work. Thank you for staring this thread. I have NEVER shared a case here. Now I'm inspired.

Today's bread/butter case:
30,31 crowns with build-ups.
emax a2 HT (sorry no final photo). All of these images were with the omnicam- I was experimenting. The omnicam camera didn't do it justice at the end.
Used isolite, cord, laser, prep, build-up with flowable filtek composite to level out undercuts.
At the try in you can see she started bleeding again. She is on plavix and had a nice huge blob of blood sitting in between 30 and 31. I Packed 3m retraction paste while sintering. Problem solved
Seated the crowns with clean and boost (apex) to clean the preps, scothbond ultimate. interface and SBU on the crowns. Seat with relyx ultimate. Also did occlusal on 29- etch, SBU and sonicfill.
About 1.75 hours start to finish. Zero occlusal adjustments, zero adjustments at try in.

#30 full coverage, #31 3/4 crown
Really conservative prep #30, Emax A2. Cemented with Variolink Esthetic DC. #31 emax A2 HT onlay (did this a while ago, would have now do cerasmart in these situations)





#3 Onlay. A2 HT Cerasmart. Cemented with Variolink Esthetic DC.









After the doing the crn posted previous, this was my next routine tx.
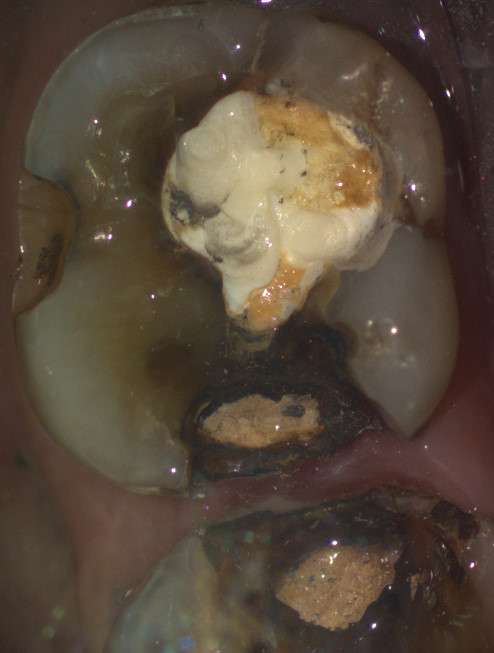
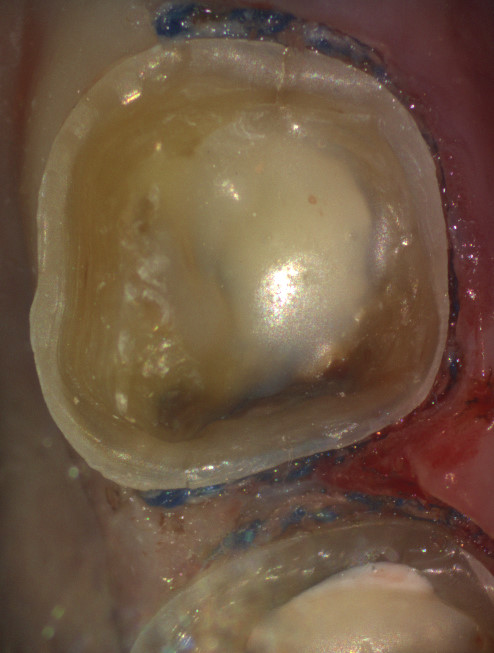
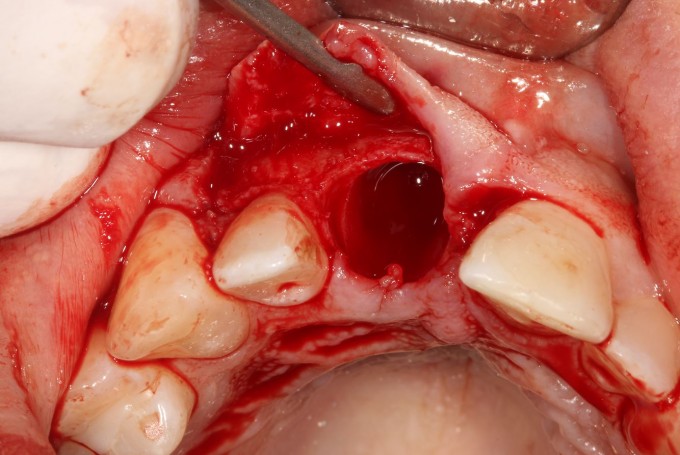
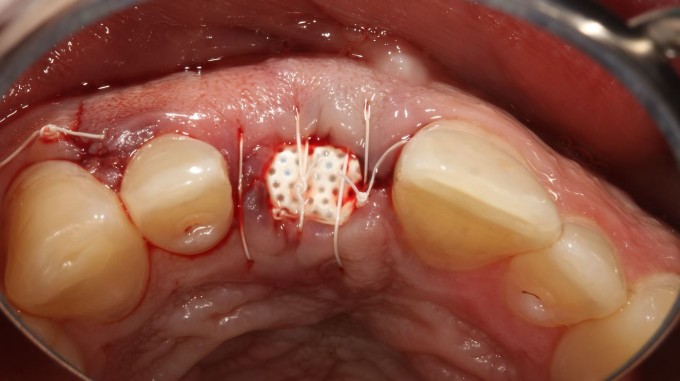
Pt Fx #8, unrestorable. Ext root, graft, cytoplast membrane, suture. I'll remove the membrane in 4 weeks, wait 2 more mos then CBCT, cerec scan, CG2, implant.Restore with cerec. Note: pt did not want to do immediate implant.




After doing 8 veneers this morning I was pretty shot. This nice old lady walks in with the lingual of #8 broken. Biocopied the good part of the tooth and made her a new emax in under one hour. My vita easyshade failed me a bit here as the final crown is too light.



And to finish out my day, some more routine cerec work. #2 fractured old composite filling, removed, tooth prepped, eMax crown bonded with Variolink.




On 4/6/2017 at 5:26 pm, Jeff Johnson said...And to finish out my day, some more routine cerec work. #2 fractured old composite filling, removed, tooth prepped, eMax crown bonded with Variolink.
Jeff,
So glad to see that you "DO" work every now and again and haven't forgotten your skills in all your excursions!
Great looking stuff!
Dan
This is truly day to day work
I had an 83 year old lady referred by OS we use for everything. He had placed implant in #10 because as she said it broke off entirely. Based on other teeth large composites likely and previous endo. She came in to see me about it and other teeth. The implant won't be ready to restore until about May. He also placed EV not knowing for sure she would come to me, so no tibases yet. All this to say I did these 3 crowns this morning before I left for Phoenix for ACCEPT tomorrow and Saturday. The photos were taken just after initial clean up and as you can see tissues weren't initially great so some bleeding( I would have waited to take longer but I wanted something fresh to show ACCEPT people what could be done)
She was ecstatic. We had told her initially 2.5- 3 hours. When we were done in about 1:40 she was so happy and made her more ready to get implant restored. FYI I also did a scan completely with an Astra scan post so we are ready to send out for abutment at least when implant ready.
I know I am not the best at stain glaze etc but these are Vita Mark II 4M2 #11 and Cerec C block (Vita) C4 12 13. Also blocks polished only. Go ahead give me the critiques





On 4/5/2017 at 8:44 am, Kunal Lal said...So here is my contribution to this thread.
Q: What happens when you designate Scan post instead of Tibase for an implant restoration?
A: You get a patient that's 'long in the tooth'
Sorry
Too funny! Great thread!

On 4/7/2017 at 8:19 am, Carrie Polster said...N
Now that's better! Empress!
Carrie, Nice work and nice pics, glad you got that DSLR.

16 y/o, athletic injury, asymmetric centrals, s/p endo and post/buildup. Empress A1 multi, with some hypocalcification staining added, placed with neutral Variolink. 



I'll get better at posting. Here is an onlay placed on #3 in February, 2008. It is Empress Cad. It looks surprisingly good for a 9 year old glass ceramic onlay. The margins aren't ditched.

JMJ
![]()
The patient shows up for the appointment, mentions the one in front of the one I'm 'sposed to fix has been sensitive - stop me if you've heard this one.
Preop



Prepped the first one, located the leak on the second and snapped a photo for the patient to see while checking hygiene.

Realized I needed to prep a crown for #4 and took a gulp. The patient want me to do it today because they don't have a lot of spare time and they are happy to pay our fee, "can you do it today?" Three is already in the mill (darned efficient assistants). What to do? Three was made to fit the existing distal of four; how about Ghost Contact (Sarmen) technique?
The assistants exported, imported, and managed the files to get ready to scan while #4 was being prepped.


Quickly took extra blood pressure medication, fast milled #4 with Cerasmart, checked hygiene, came back to bond #3, 4.
The add-a-crown technique, courtesy of Cerec and the amazing dental assistants I get to work with ![]() .
.
God Bless
matt
