
Immediate implant instead of the crown we planned.

We all have this happen to us, our schedule laid out the way we want for a productive smooth running day, then something happens to throw a wrench in it. My Wednesday morning I had a crown on #8 to start the day and then an implant right after that. The crown patient came in with the crown #5 off at the gum line.

Now we have a problem. I only have one room set up for implant surgery. I don't have time to make a guide for this case, get the tooth out and place the implant before my next patient comes in and needs her implant placed. So the decision was made to go ahead and extract and place the implant free hand. Normally implant surgery is done with a guide in my practice. There are times that either the guide doesn't fit or fabrication of the guide is not feasible. This is why it is important for doctors to have the surgical abilities to place an implant free hand.
The plan in this case was to split the roots and place the implant in the interseptal bone to get primary stability.
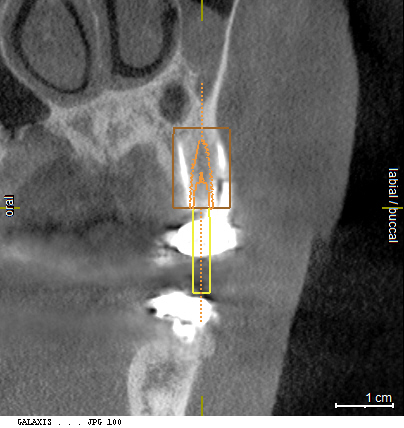
The roots were sectioned with a high speed hand piece with a long shank surgical bur. This serves to purposes. One is to make the removal of the roots easier. Secondly it also gives a guide for the drill to not kick buccal or lingual during preparation of the osteotomy. Now all we need to do is manage the mesial distal position during the osteotomy preparation. Having the CBCT did however help show where we needed to section the tooth and how deep to go to make sure that the tooth was sufficiently. Unfortunately due to the time constraints trying to get the case done before my next patient gets here I didn't get a photo of the sectioning. Once the osteotomy was finished the roots were removed atraumatically. The implant was then placed with 35+ncm of torque and the root areas were grafted with cortical/cancellous

Could this case have been done guided, sure but I would have either had to reappoint the patient(they are not the most reliable patient) or run behind and make my next implant patient wait. As it was the patient got the tooth extracted and the implant placed and we were on time for our next patient. Guides are great but ultimately the surgeon needs the skills to know how the surgery should go even if they don't have a guide.


On 1/22/2017 at 5:17 pm, Darin O'Bryan (Faculty) said...Could this case have been done guided, sure but I would have either had to reappoint the patient(they are not the most reliable patient) or run behind and make my next implant patient wait. As it was the patient got the tooth extracted and the implant placed and we were on time for our next patient. Guides are great but ultimately the surgeon needs the skills to know how the surgery should go even if they don't have a guide.
Could not agree more Awesome job threading the needle!

Not an easy situation to free-hand but you nailed it Darin so kudos to your skills.
If it was me I would have temped #5, taken a scan for the guide, stuck with my plan to do the crown #8, and then done the implant guided at the next visit (instead of now doing the crown at the next visit)....Life is too short to stress yourself out.
Farhad

paraphrasing a line that I love from one of Dr Butterman's posts ........
.....you were guided by your brain in this surgery!![]() .......skillz
.......skillz
On 1/22/2017 at 11:19 pm, Farhad Boltchi (Faculty) said... Not an easy situation to free-hand but you nailed it Darin so kudos to your skills. If it was me I would have temped #5, taken a scan for the guide, stuck with my plan to do the crown #8, and then done the implant guided at the next visit (instead of now doing the crown at the next visit)....Life is too short to stress yourself out. Farhad
Less stressful doing a single central, only a surgeon would make that statement![]() . I could have done that but we may not even do the crown this year due to finances and insurance and as I stated the patient isn't the best for showing up. If I temped him and did the crown(which was being done due to a fractured large fill) He would likely wait until it either came off again or started hurting. When he presented he had no apical pathology but decay into the canal. The extraction was only going to get harder if he waited. There are some patients you just know are not good at follow up.
. I could have done that but we may not even do the crown this year due to finances and insurance and as I stated the patient isn't the best for showing up. If I temped him and did the crown(which was being done due to a fractured large fill) He would likely wait until it either came off again or started hurting. When he presented he had no apical pathology but decay into the canal. The extraction was only going to get harder if he waited. There are some patients you just know are not good at follow up.
This post came about from a conversation I had with an OMFS that runs a study club I spoke at last week. We were talking about how there are some out there that make the claim that with guided surgery you can take a doctor from never having placed an implant to perfect placement because they are using a guide. The problem is the clinician still needs to know how to do surgery. Even with a guide in this case you would need to know what it felt like to drill through tooth vs. bone, how to remove the root tips atraumatically to preserve the facial plate, get enough primary stability and how to graft the site. To many people out there are making weekend implantologists out of clinicians after a weekend course.

On 1/23/2017 at 9:48 am, Darin O'Bryan (Faculty) said......There are some patients you just know are not good at follow up....
Ain't that the truth - and it does play a role in treatment planning!
Tom

On 1/23/2017 at 9:48 am, Darin O'Bryan (Faculty) said...On 1/22/2017 at 11:19 pm, Farhad Boltchi (Faculty) said... Not an easy situation to free-hand but you nailed it Darin so kudos to your skills. If it was me I would have temped #5, taken a scan for the guide, stuck with my plan to do the crown #8, and then done the implant guided at the next visit (instead of now doing the crown at the next visit)....Life is too short to stress yourself out. FarhadLess stressful doing a single central, only a surgeon would make that statement
. I could have done that but we may not even do the crown this year due to finances and insurance and as I stated the patient isn't the best for showing up. If I temped him and did the crown(which was being done due to a fractured large fill) He would likely wait until it either came off again or started hurting. When he presented he had no apical pathology but decay into the canal. The extraction was only going to get harder if he waited. There are some patients you just know are not good at follow up.
This post came about from a conversation I had with an OMFS that runs a study club I spoke at last week. We were talking about how there are some out there that make the claim that with guided surgery you can take a doctor from never having placed an implant to perfect placement because they are using a guide. The problem is the clinician still needs to know how to do surgery. Even with a guide in this case you would need to know what it felt like to drill through tooth vs. bone, how to remove the root tips atraumatically to preserve the facial plate, get enough primary stability and how to graft the site. To many people out there are making weekend implantologists out of clinicians after a weekend course.
Well put, implant surgery is a science and and art. I see people get all the equipment and put them exactly where they want but do not understand where they need to be....
