
#8 Endo/ Post/ Core/ Crown- What would you have done?

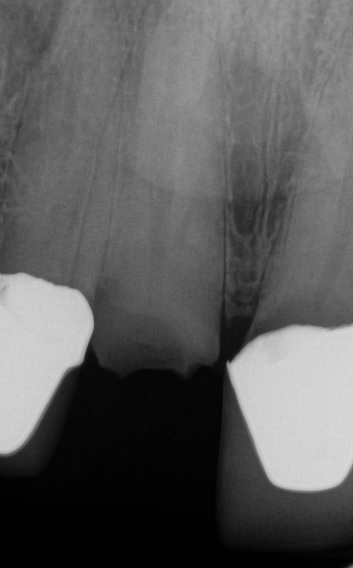
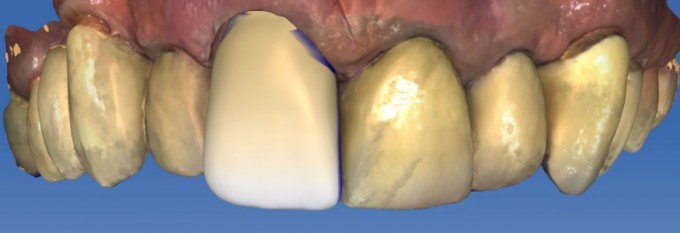
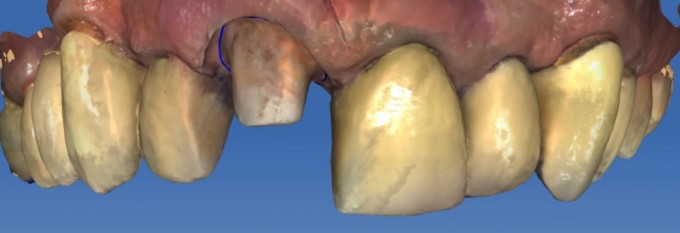
This happens in all of our practices. A long time patient schedules an appointment yesterday for a "chipped tooth" I walk in to the op and see the case below. As you can see cerec handled the case as we would all expect. I spent time discussing the options with the patient to include:
1) extraction, implant, abutment and crown
2) extraction, Chairside FPD
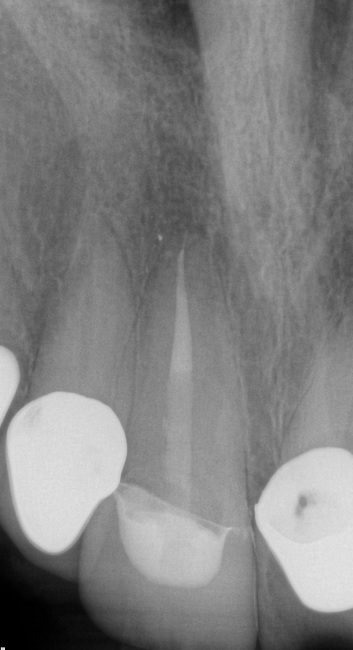
3) endo, post/core, crown
As I presented the options, I even stated that option number three is becoming outdated in its philosophy and that dentistry as a profession is moving away from the less predictable long term prognosis of the endo/post/ core. I also stated that I did not like option two because of the uncertain condition of #9. The patient chose option #3. I know him very well and as I stated, he has been a patient of mine for twenty years. So I asked him why he chose that option. His answer, "I am 80 yrs old, I have had 17 surgeries in the last 9 years, and I just don't want another one if I can avoid it." Can't argue with that at all. So the question is, what would you guys have done? With all of the technology we have at our fingertips, are we forgetting traditional dentistry?




Dave, you're brave. Do you have a prep photo by any chance? Did you consider to do partial extrusion with partial extraction method? Gregory
On 12/21/2016 at 7:53 am, Gregory Mark said... Dave, you're brave. Do you have a prep photo by any chance? Did you consider to do partial extrusion with partial extraction method? Gregory
LOL...I did consider extrusion and offered it. Patient wanted quick, simple and definitive (even if short term). I will keep my fingers crossed. Merry Christmas Gregory. Been way to long!

That's how I would have handled it. As long as you take care of him if it fails prematurely, what's the harm? Nice case.

That is a beautiful result and nothing wrong with this option at all, especially for an 80 year old. He has a very deep bite and I would have certainly tried to move the excursive contacts onto the natural teeth a bit, but I think this is a great treatment for your patient

On 12/21/2016 at 7:57 am, Bob Conte said...That's how I would have handled it. As long as you take care of him if it fails prematurely, what's the harm? Nice case.
+1

Tough situation and a great immediate result. I'd say that as long as there is some sort of ferrule onto natural tooth (past the fracture), you have a chance. Without that ferrule, not sure it will be a long enough lasting fix. NO harm in trying though, as the FPD isn't excluded because of your efforts. I'd do it if my patient expected me to "give it a go."

Dave
I think you did the right thing. The patient was informed of the options and as long as you had 2-3mm of ferrule and control the excursive movements over that tooth your are good. Most likely you will get chronological success. If not worse case scenario it breaks you don't charge him for the crown you just did and due a FPD from 7-9. One of the beautiful thing about CEREC is we can do this and the lab fee is not crippling if things go south.
On 12/21/2016 at 8:21 am, Ernie Johnson said...Tough situation and a great immediate result. I'd say that as long as there is some sort of ferrule onto natural tooth (past the fracture), you have a chance. Without that ferrule, not sure it will be a long enough lasting fix. NO harm in trying though, as the FPD isn't excluded because of your efforts. I'd do it if my patient expected me to "give it a go."
Darin and Ernie,
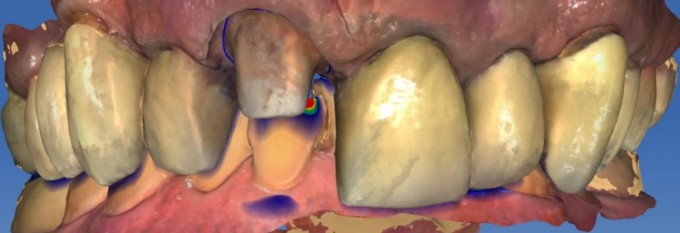
We were able to get a good ferrule on the palatal and about 1-1.5 mm on the facial so i feel pretty comfortable. Great to be talking about the merger of traditional dentistry with today's technology to make the results that much better.

On 12/21/2016 at 8:18 am, Daniel Butterman said...On 12/21/2016 at 7:57 am, Bob Conte said...That's how I would have handled it. As long as you take care of him if it fails prematurely, what's the harm? Nice case.
+1
+2 a fully informed patient will know you have done all that is possible to do...within the limitations he has set forth...
Mark

On 12/21/2016 at 7:57 am, Bob Conte said...That's how I would have handled it. As long as you take care of him if it fails prematurely, what's the harm? Nice case.
+3...Nice job Dave. I think you did what I hope we would all do. Inform our patients of their options and expected prognosis and let them decide.



I have seen a few of these cases and have gone this route a couple of times. It does make me feel like I am getting overly dependent on adhesives and bonding when there is lacking ferrule. I am interested in what people use as a benchmark for premature failure or success in this situation? If it lasts 5 years is that a success?
On 12/21/2016 at 6:27 pm, Grady Twohig said... I wish you had a photo of the prep. Can you do a screenshot of the scan at least?
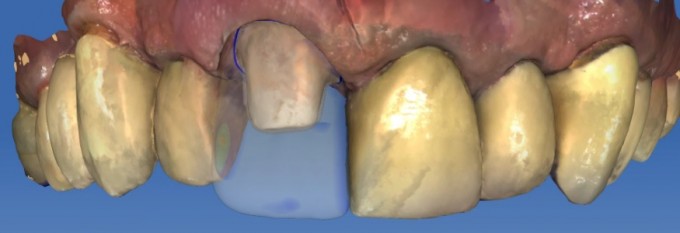
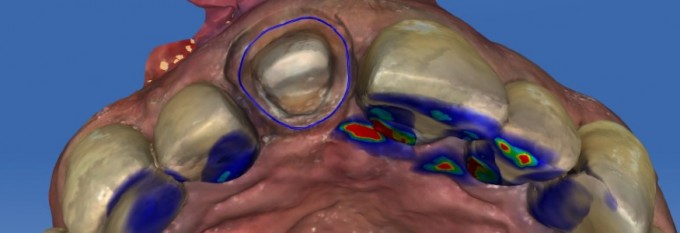
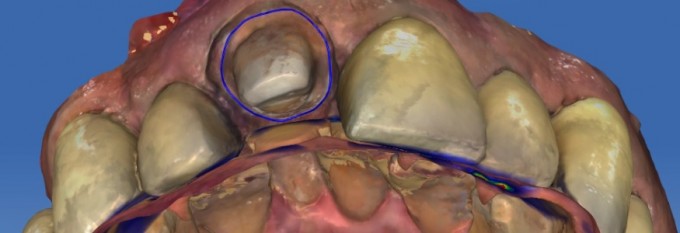
I will post a few shots of the prep tomorrow. The occlusion was so tight because of the deep bite I was lucky to get what I did for height and geometry of prep. I will post though for sure. Check back in am.
On 12/21/2016 at 8:55 pm, Matthew Sandberg said... I have seen a few of these cases and have gone this route a couple of times. It does make me feel like I am getting overly dependent on adhesives and bonding when there is lacking ferrule. I am interested in what people use as a benchmark for premature failure or success in this situation? If it lasts 5 years is that a success?
Without a doubt we are getting dependent on adhesives. But in this case it makes me feel way MORE comfortable. I was able able to bond in the fiber post and was happy with the prep height I did get. I think the great thing about adhesives in this case is that they give us a little reassurance that we could do more than just the traditional "cements" used to offer. I will post the prep screen shots tomorrow and a few pics with the lower in occlusion. That really brings to light the challenges these cases pose.
I was able to get some ferrule on the prep but haven't decided what will make this case a success yet. As of now I am two days out so just happy it didn't fail with the first meal. Great discussion for sure because I bet we could get 100 different thoughts on what will eventually determine the success of this case.

Dave,
I've done a few of these with no ferrule. One or two have been successful, but most of them fail. The post snaps off clean and the core and crown are either swallowed or spit out. I inform the patient of the short service life of these restorations and very few patients I have seen choose to go this route. I treated an upper first molar of the wife of a friend of mine with three fiberglass posts and a core buildup and crown. She got 6 years out of it. If the patient wants to try it after being duly informed, I will oblige as you did, but with no guarantees. I would also favor extrusion first, but most patients want the quick fix.
On 12/21/2016 at 9:27 pm, Charles LoGiudice said...Dave,
I've done a few of these with no ferrule. One or two have been successful, but most of them fail. The post snaps off clean and the core and crown are either swallowed or spit out. I inform the patient of the short service life of these restorations and very few patients I have seen choose to go this route. I treated an upper first molar of the wife of a friend of mine with three fiberglass posts and a core buildup and crown. She got 6 years out of it. If the patient wants to try it after being duly informed, I will oblige as you did, but with no guarantees. I would also favor extrusion first, but most patients want the quick fix.
The down side in a case like this is the experience we all have with it. I think we all walk that line sometime between our experiences and the patients decision based on what they want quickly. In this case I felt I provided the patient with his options and the prognosis of each. At that point, as long as we do nothing ethically wrong, I believe we work for the patient and should do our best to accomplish a great clinical result.....no matter how long it lasts. As you guys can see, even after the core was built up there was little room for more length because of the occlusion. Unfortunately, even with proper instructions, and minimal functional occlusion, Long term prognosis may be questionable. I wonder how many of my gray hairs are due to cases like this? LOL
