
Another Lightwalker laser one-piece e.Max crown removal

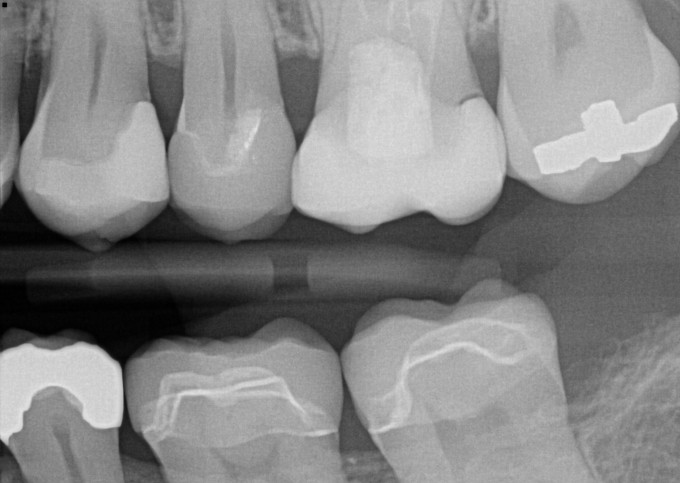
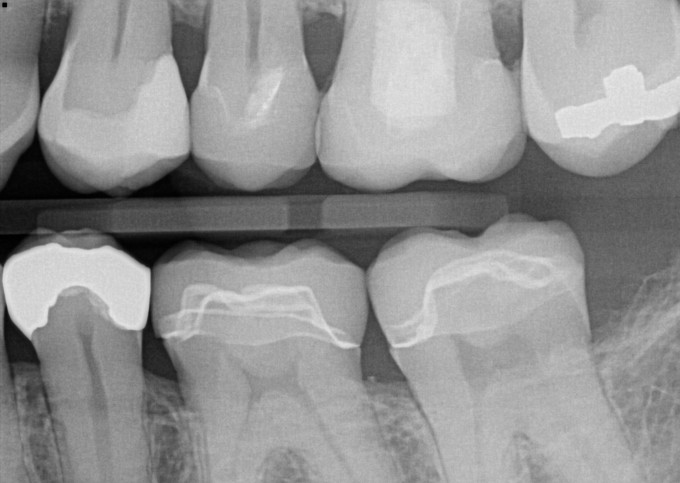
Sometime this past summer, I can't remember exactly when, one of our faculty showed a case and commented on the difficulty of removing an e.Max crown by sectioning it with a bur. People comment from time to time about how it is often necessary to prep e.Max crowns off because the bonding resins we use provide such a strong bond. I fractured the tooth with one of the first ones I tried to remove because I did not section it into enough pieces. Then, an article in Dentistry Today, a "throw away journal" as we are fond of calling some of the periodicals we get in the mail, changed my life--a slight over statement there. Dr. Jeffrey Cranska presented his protocol for debonding e.Max crowns using his Fotona Powerlase, removing the restorations in one piece. I tried it the next time I had to remove a bonded ceramic crown, and it works! 3 to 5 minutes bathing a crown in ErYAG laser energy certainly beats 15 to 20 minutes (or more) sectioning and chipping away a ceramic crown. Admittedly, the investment in the laser and the necessary training requires more justification than removing ceramic crowns in one piece. I use mine for endodontic irrigation, perio (including frenectomies, ginvgivectomies, and I have even done a couple of torus removals), and preparing small carious lesions. 90% of my pedo is done with my Lightwalker laser and no anesthetic, and adult patients are more than tickled pink when they walk out of my office after receiving a "filling" and they are not numb at all. This case is one of my failures--an open distal margin on a #14 Celtra Duo crown. My conscience wouldn't let me kick this can down the road and when the crown was removed, decay was found on the distal axial wall of the preparation. This case was done as warranty work, as I call it. Don't ask me why the replacement crown is e.Max. There was nothing wrong with the Celtra Duo crown other than the open margin, which was not the fault of the material. I did remove that bonding resin under the distal contact before the patient was dismissed. PS Fotona gave me a list of 20 CEREC docs, all of whom are on this forum, including Skrammy, and they want me to try to try to sell a few machines. I told them that my chances of doing that are slim and none. 

I've been wanting to try this but didn't know the settings. I found the Cranska article and badabing - there are the parameters to use! Thanks for the info!!
Ray,
Cranska uses the R14 handpiece with a 1mm x 8mm Sapphire tip. I use the R02 tipless handpiece with the same settings.

If a laser salesperson ever shows up at my door on the same day I removed a bonded emax they would have an easy sale. I absolutely hate cutting them off. It is usually for the exact same reason you did Chuck with an opening due to lack of cement or too tight of contact.
I thank you for your testimonial. I would like to know if any of the other lasers can do this procedure. There was an article in the January 2016 issue Journal of Prosthetic Dentistry about this exact technique.
This technique could come in handy in ten years when we start seeing some of the bonded restorations come back with recurrent caries just like we do with PFM's not. Thanks for the tip's Chuck. Keep them coming. You are the best.
On 11/1/2016 at 7:35 am, Aaron Tinkle said...If a laser salesperson ever shows up at my door on the same day I removed a bonded emax they would have an easy sale. I absolutely hate cutting them off. It is usually for the exact same reason you did Chuck with an opening due to lack of cement or too tight of contact.
I thank you for your testimonial. I would like to know if any of the other lasers can do this procedure. There was an article in the January 2016 issue Journal of Prosthetic Dentistry about this exact technique.
This technique could come in handy in ten years when we start seeing some of the bonded restorations come back with recurrent caries just like we do with PFM's not. Thanks for the tip's Chuck. Keep them coming. You are the best.
Aaron,
I understand that this can be done with the Biolase Waterlase as well. It has to be an Erbium hard tissue laser as far as I know. Aaron, give me your address and I can get a laser sales person to your office faster than you can imagine.

You're absolutely right Charles. I've been using the Waterlase iPlus to remove ceramics for years with great success. You can literally remove a veneer in about 10 seconds. Another great use for for these laser systems.
Luke

I've found the settings to not be overly critical. The trick is to get energy penetration to the bond layer for disruption. If you've ever used a hard tissue laser to remove composite material you'll know how little energy is required to remove it at a very quick pace. I usually start at 4W, 15hz for a thin veneer and if it doesn't "pop off" in the first few seconds then I increase the energy. For a thick crown, 8W, 15 hz and again, simply adjust as necessary. Having the tip in very close proximity to the surface at 90 degree angle works best, unlike a typical hard tissue preparation where the tip needs to be further away from the surface.

Between this function for removing cerecs and potential for sleep apnoea application I'm very tempted to move on one of your lasers. I'll try and have the local rep cut you in on his commission for promoting the laser (LOL).
Any update on the palate laser treatments Charles?
Damian,
There is more to it than Nightlase. There is also Smoothlase, which is facial wrinkle ablation without Botox or Dermal Fillers. I started slowly after the training. I have had Nightlase done for me by a retired friend from dental school who was doing Nightlase when he retired. In my case, my wife says I don't snore any more. I was diagnosed with Sleep Apnea by a sleep physician. I can't tolerate a c-Pap. I tried Smoothlase for my wife and it didn't go well. At the training, Dr. Shiffman was pretty adamant about the settings and the protocol. The settings were too much for my wife. I am doing Nightlase for my front desk lady. The settings were tolerable but the number of bursts per aiming beam spot were too much for her so we reduced the number of bursts per spot from 6, which was presented in the training, to 4. Today, I did the fourth session for her and I also reduced the milli-joules/second. After 4 visits with a modified treatment protocol her Mallampati score has has been reduced from a 4 to almost 2. I figure we will need 2 more sessions to achieve the desired results. I also started Nightlase for my Patterson rep today. We tried with him a month ago and he couldn't tolerate it. The laser bursts were too hot for him. I reduced the milli-joules/second even more for him than for my front desk lady and he tolerated it satisfactorily. The bottom line is that I have learned that each patient is different and the amount of laser energy used for each patient needs to be titrated. Dr. Shiffman tends to present the protocol as rigid and unchangeable. If the settings or the protocol are modified, the only consequence is that the number of sessions is increased. Now that I have some experience and am rolling with it, my wife is willing to give Smoothlase (wrinkle smoothing) another try. I will definitely reduce the millijoules/second for her. I have found that maybe the most serious challenge is how to charge for laser therapy. Dr. Shiffman practices in Jupiter, Florida. That is a snowbird and retirement community surrounded by many high-end gated subdivisions. That area is populated by people with some serious assets. His basic charge is $500/session, and he uses three sessions with his protocol. There is no way that will fly in my area. I am thinking that most people will require a lower beam intensity than Harvey prescribes and thus, more patient visits will be required to generate the desired results. $500/visit, $1500 for the regimen is more than my traffic will bear. Also, people who are using a c-Pap require more appointments--5 or 6--and Harvey charges a straight $500/visit. He does not cap his fee for treatment. I apologize for the long answer but this is not a simple topic. The bottom line is that, after training, there is a learning curve and there are some issues to work out. I have accumulated enough experience in the pro bono learning phase and I am now ready to market Nightlase and Smoothlase and start treating some fee for service patients. In summary, that is how my experience with Nightlase and Smoothlase is progressing. BTW, I was offered no benefits or commission for any sales I might generate. I started this thread because I believe in the technology.

Dr. Chuck,
What were the settings you have been using to remove Emax? I have a Powerlase from Fotona, which was the unit prior to the Lightwalker and have been aware that it could be used to remove porcelain but always thought it was more for feldspathic restorations and not emax.
Thanks,
Don
On 11/1/2016 at 5:55 am, Charles LoGiudice said...Sometime this past summer, I can't remember exactly when, one of our faculty showed a case and commented on the difficulty of removing an e.Max crown by sectioning it with a bur. People comment from time to time about how it is often necessary to prep e.Max crowns off because the bonding resins we use provide such a strong bond. I fractured the tooth with one of the first ones I tried to remove because I did not section it into enough pieces. Then, an article in Dentistry Today, a "throw away journal" as we are fond of calling some of the periodicals we get in the mail, changed my life--a slight over statement there. Dr. Jeffrey Cranska presented his protocol for debonding e.Max crowns using his Fotona Powerlase, removing the restorations in one piece. I tried it the next time I had to remove a bonded ceramic crown, and it works! 3 to 5 minutes bathing a crown in ErYAG laser energy certainly beats 15 to 20 minutes (or more) sectioning and chipping away a ceramic crown. Admittedly, the investment in the laser and the necessary training requires more justification than removing ceramic crowns in one piece. I use mine for endodontic irrigation, perio (including frenectomies, ginvgivectomies, and I have even done a couple of torus removals), and preparing small carious lesions. 90% of my pedo is done with my Lightwalker laser and no anesthetic, and adult patients are more than tickled pink when they walk out of my office after receiving a "filling" and they are not numb at all. This case is one of my failures--an open distal margin on a #14 Celtra Duo crown. My conscience wouldn't let me kick this can down the road and when the crown was removed, decay was found on the distal axial wall of the preparation. This case was done as warranty work, as I call it. Don't ask me why the replacement crown is e.Max. There was nothing wrong with the Celtra Duo crown other than the open margin, which was not the fault of the material. I did remove that bonding resin under the distal contact before the patient was dismissed. PS Fotona gave me a list of 20 CEREC docs, all of whom are on this forum, including Skrammy, and they want me to try to try to sell a few machines. I told them that my chances of doing that are slim and none.
Dr. Chuck, This is why I read most everything you post. Your passion and ethics are unmatched.
BTW I have both a AT powerlase and an iplus. Use them both everyday. People ask if there is something that is worth the investment I tell them a hard/soft tissue laser and OmniCam... Oh and of course cerecdoctors.... Have a great Holiday....
