
Difficult Lateral Incisor implant restoration with grafting

Here is a case that I posted about a year ago that we are now ready to restore. It was a difficult case that we have been working on for awhile and I thought I would post it since it is turning out better than expected.
This patient came to me as a new patient on a second opinion referral to evaluate #10 for an implant. Here previous dentist said she was not a candidate for implant due to no bone and wanted to do a bridge.
Here is her preop situation:


We extracted #10 and waited two months to go back in for bone grafting. We used bone morphogenic protein and a titanium mesh technique (non-demineralized allograft and growth factor).
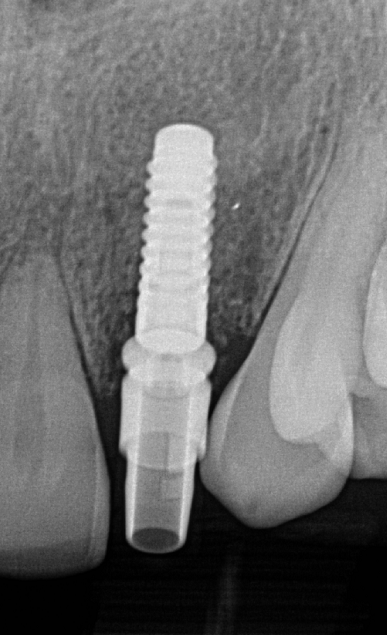
After 6 months we removed the mesh and placed a 3.3 Straumann Bone Level implant in the site.
When we went to form the tissue with a Teliocad abutment block, we could not get the titanium base to seat due to bone interference (normal with a narrow diameter implant and titanium base).
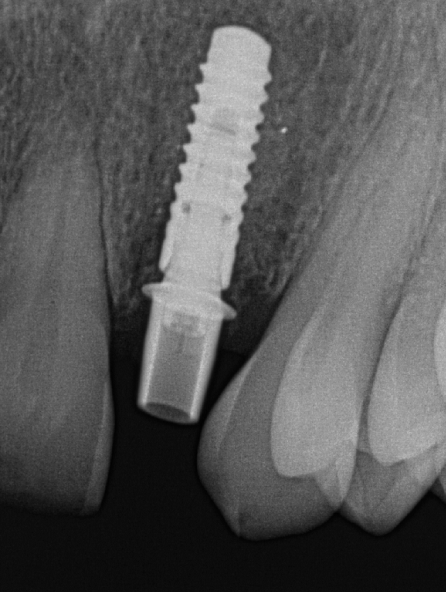
Since she had a lot of room, we used the Straumann Guided bone profiler and removed some of the shoulder of titanium base for the provisional

After 3 weeks of healing, here is the final tissue position/healing ready to restore.


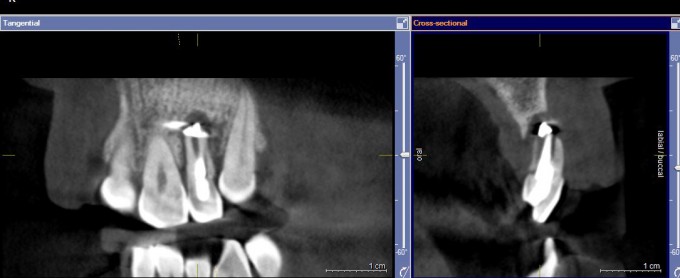
I imaged today for the final and the scanpost seated with zero issue due to the bone profiling. I will post the final after seating next week.

Nice work on getting the tissue to be supported. Slow and steady wins the race. We tend to try and rush things to much and then end result is a compromise. Really nice work.


Mike, can you tell me more about the mesh being left for 6mos for the bone development? Material, pics?, etc.
Thanks,
JJ
The oral surgeon I work with did the surgery. I will let Farhad give details on the technique since I do not do that kind of surgery

Mike, I would add soft tissue grafting to cover greyish color of the gum and improve papilla. I would a little horizontal cut without raising periosteum and push soft tiissue graft towards gingival crevice , sling sutures, make sute that papillas are free to move incisaly. Gregory
That was an option we talked about Gregory... But she has a lower lip line and didn't think it was necessary for additional surgery.
I agree though. If we wanted perfection in this, j would have done this as well.
This case is a huge success in my mind based on our starting point.

I don't use the titanium mesh technique (since I use the SonicWeld reconstructive technique) but here are the details:
A wide flap reflection with vertical releasing incisions, Debride defect, Cut a piece of titanium mesh to the shape of the desired ridge contour, Screw titanium mesh to the palatal aspect (or alternatively to the buccal aspect), Prepare InFuse BMP-2 by soaking the supplied collagen sponges in the BMP-2 fluid, Mix the mineralized allograft (such as Straumann allograft or MinerOss for example) with the soaked collagen sponges like rolling a burrito, Apply the bone graft/collagen sponge mixture to the defect site reconstructing the ridge contour, Fold the titanium mesh over the crest to the buccal side (or the palatal side) and screw it down, Optionally (most people do this) put a resorbable membrane on top of the mesh, Perform a generous periosteal release and coronally advance the flap for complete tension-free coverage of the reconstructive complex, Suture.
The disadvantage of the titanium mesh technique and why I don't use it is that there is a high chance of exposure of the mesh (25% in experienced hands). The semi-circular area in Mike's case may have been an area of mesh exposure that granulated in secondarily. Typically the area of mesh exposure doesn't get infected but it leads to soft tissue defects. The other disadvantage is that it requires a larger flap to dissect the mesh out and remove it at second stage.
An alternative easier mesh technique is to send a CT scan of the case to a company in Germany. They will digitally simulate the ideal ridge contour, fabricate a corresponding titanium mesh (don't know if they print this mesh), and send the pre-formed mesh to the surgeon. This shortens the surgery since the mesh is already pre-formed.
The mesh technique is very technique-sensitive and requires experience. Obviously the Oral Surgeon in the case above was very skilled and achieved a beautiful hard and soft tissue foundation for Mike. Now it's just up to Mike not to screw it up...lol.
Farhad

I would probably not do a connective tissue graft in this case even if the patient had a high lip line.
A connective tissue graft is not going to improve the height of the papillae and the buccal tissue appears quite thick to me already...So there is nothing to be gained from a CTG IMO.
Some loss of papillary tissue height is to be expected when a major reconstructive procedure like this is performed. Some or all of the papillary height may come back over time (per studies it can take up to 2 years) as long as the embrasures are not closed off....And if not then it just needs to be accepted.
Farhad
Farhad-
Can you describe the sonic weld technique and why this is easier.
I've been working with the same oral surgeon for a very long time. He is incredible and hugely supportive and interested in the digital restorative techniques that I use.
On 2/8/2016 at 12:45 pm, Mike Skramstad (Faculty) said... Farhad- Can you describe the sonic weld technique and why this is easier. I've been working with the same oral surgeon for a very long time. He is incredible and hugely supportive and interested in the digital restorative techniques that I use.
The SonicWeld technique is technically easier with regard to the surgical procedure, exposures are easy to handle, and there is no need to remove the barrier as it is resorbable (the second stage can even be done flapless).
Here are the details:
Farhad

Farhad,
So I have a surgeon that I used to work with a lot more who places Straumann implants. He is a very talented surgeon, but not a fan of Ti-base. When I have asked him to profile the bone in some cases, he just argues with me and says that I should use a custom lab fabricated abutment. As you would imagine, I have shifted my referrals to another surgeon who is very interested in digital technology and wants to understand what I am looking for from a restorative perspective. I definitely under the cons of Ti-base and know you are a huge fan in the NC cases, but maybe could you explain why he is so adverse to profiling bone in cases to help the tibase seat completely? Thanks
Dan
On 2/8/2016 at 12:58 pm, Daniel Wilson said...Farhad,
So I have a surgeon that I used to work with a lot more who places Straumann implants. He is a very talented surgeon, but not a fan of Ti-base. When I have asked him to profile the bone in some cases, he just argues with me and says that I should use a custom lab fabricated abutment. As you would imagine, I have shifted my referrals to another surgeon who is very interested in digital technology and wants to understand what I am looking for from a restorative perspective. I definitely under the cons of Ti-base and know you are a huge fan in the NC cases, but maybe could you explain why he is so adverse to profiling bone in cases to help the tibase seat completely? Thanks
Dan
Dan,
This can be a lengthy discussion but I will try to shorten it:
From a biological point of view it is always best to keep the restorative interface as far away from the bone as possible. Hence the need for narrow tibases (see Mike's modification above) and tibases with a 2mm height (a la Conelog). A custom titanium abutment (what the surgeon may be referring to) is biologically sound as well since it displaces the abutment-restoration interface more coronally.
However, using a titanium custom abutment doesn't alleviate the need for bone profiling as that is more dependent on the need for a correct emergence profile....And the tibase restorative workflow (be it our CEREC workflow or any other tibase system) can be accomplished in a biologically sound way as well as has been demonstrated by Mike and many others over and over again.
Farhad

On 2/8/2016 at 12:57 pm, Farhad Boltchi (Faculty) said...On 2/8/2016 at 12:45 pm, Mike Skramstad (Faculty) said... Farhad- Can you describe the sonic weld technique and why this is easier. I've been working with the same oral surgeon for a very long time. He is incredible and hugely supportive and interested in the digital restorative techniques that I use.The SonicWeld technique is technically easier with regard to the surgical procedure, exposures are easy to handle, and there is no need to remove the barrier as it is resorbable (the second stage can even be done flapless).
Here are the details:
Farhad
Farhad,
I saw sonic weld at a pat Allen course a few years ago. I like the idea of a resorbable membrane so you do not have to go back and remove the membrane. Is there any courses for it? And where can you get the kit? Approx cost per membrane? Thanks!
Mike nice case, that's a tough one, they can be quick sand....

On 2/8/2016 at 12:57 pm, Farhad Boltchi (Faculty) said...The SonicWeld technique is technically easier with regard to the surgical procedure, exposures are easy to handle, and there is no need to remove the barrier as it is resorbable (the second stage can even be done flapless).
Here are the details:
Farhad
Darnit Farhad. You really had to show off this technique? Now I need to look into this more. That means buying more equipment and taking a soft tissue management course to manage those flaps.
On 2/10/2016 at 9:07 am, John Pasicznyk said...On 2/8/2016 at 12:57 pm, Farhad Boltchi (Faculty) said...The SonicWeld technique is technically easier with regard to the surgical procedure, exposures are easy to handle, and there is no need to remove the barrier as it is resorbable (the second stage can even be done flapless).
Here are the details:
Farhad
Darnit Farhad. You really had to show off this technique? Now I need to look into this more. That means buying more equipment and taking a soft tissue management course to manage those flaps.
John...I don't know how you fit it all in right now...you're an animal!

Really nice management and outcome, Mike. I'd love to see the post-op CBCT images compared to the pre-op, plus any surgical photos your OMFS took. It looks as though there was zero buccal plate and it sounds like you threw everything possible at this case to get a really nice result. Now, about the rest of those teeth....




Great restorative result, contour, color, etc. Really nice job. Your surgeon did a fantastic job with the facial soft tissue as well, really set it up for success. Sometimes an interdisciplinary approach can allow everyone to do what they do best.


Mike, that is nothing short of amazing. Kudos to both of you....I guess all three of you if we include the patient.
Great case Mike! Love the depth of color...how many firings to achieve that? For me, I feel like I need a minimum of two...
On 2/17/2016 at 12:20 pm, Daniel Wilson said... Great case Mike! Love the depth of color...how many firings to achieve that? For me, I feel like I need a minimum of two...
This was two fires. The second one I stained directly in her mouth

Lustre paste? How was the colour scheme? Wich color makes that bluish translucency?
great job

Thanks everyone. This case turned out to be one of my most satisfying of my career.
Luis, the stains were done with L8 (olive), L2 (white) and L5 (light blue). Really helps doing it right in the mouth
I'll assume after you stain in the mouth...you don't have any good tricks to get the crown out without messing up the work you just did....just be very, very careful??!? :)

